Retake
C23) Worsening dyspnea on exertion and leg swelling in a young female
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a patient with hypoxia.
- Review the DDx considerations in a patient with hypoxia.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating a patient with hypoxia.
History
A 28-year-old female presents with progressively worsening dyspnea on exertion, fatigue, and leg swelling for the past few months. She has experienced dizziness and fainting episodes, and is no longer able to walk up a flight of stairs without losing her breath. This is her first visit related to these symptoms.
Physical Exam
BP: 132/80, HR, RR 25, Temp 95.4, O2 saturation 92%. BMI 24. Cardiovascular exam: Cardiovascular exam reveals an augmented pulmonic component of the second heart sound, a third heart sound gallop, and a systolic ejection murmur heard best at the left sternal border. There is jugular venous distension and bilateral pitting edema in her legs.
Labs
ECG: Right ventricular hypertrophy.
Provisional Diagnosis
Select the Dx you believe is most appropriate
The patient is experiencing progressive dyspnea on exertion and fatigue, as well as exhibiting signs of right-sided heart failure, including an augmented P2, S3 gallop, systolic ejection murmur on the left sternal border, jugular venous distension, and bilateral pitting edema in the legs. These symptoms are indicative of pulmonary artery hypertension.
Well done. You were correct
Potential Acuity
What is your assessment of the likely acuity for this patient?
Well done. You were correct
Considering the chronicity of the patient's symptoms, routine evaluation is appropriate.
First Imaging Study
What is the first imaging study you will order?
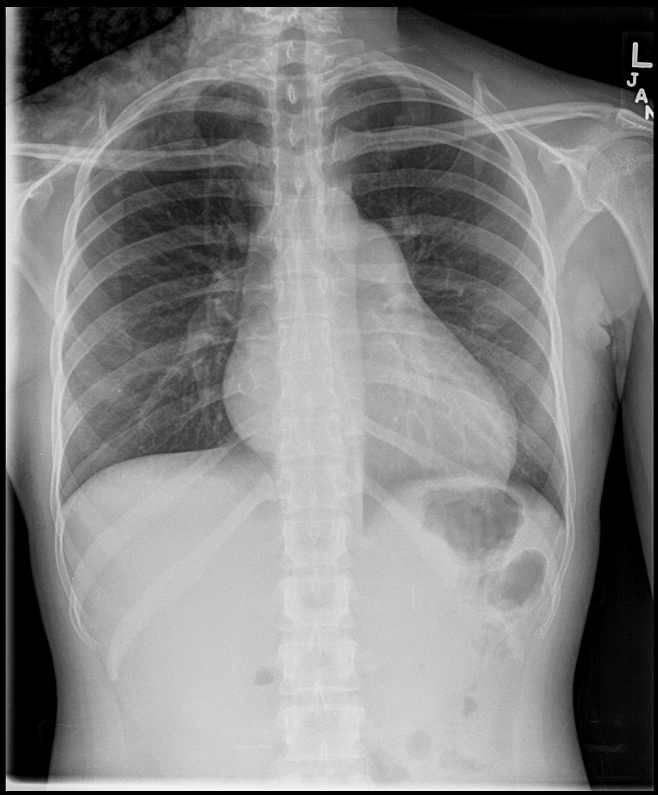
A chest x-ray is a cost-effective and quickly obtainable imaging modality that can help rule out other conditions.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
View the full study if you'd like to take a look yourself.
Second Imaging Study
What is the next imaging study you will order?
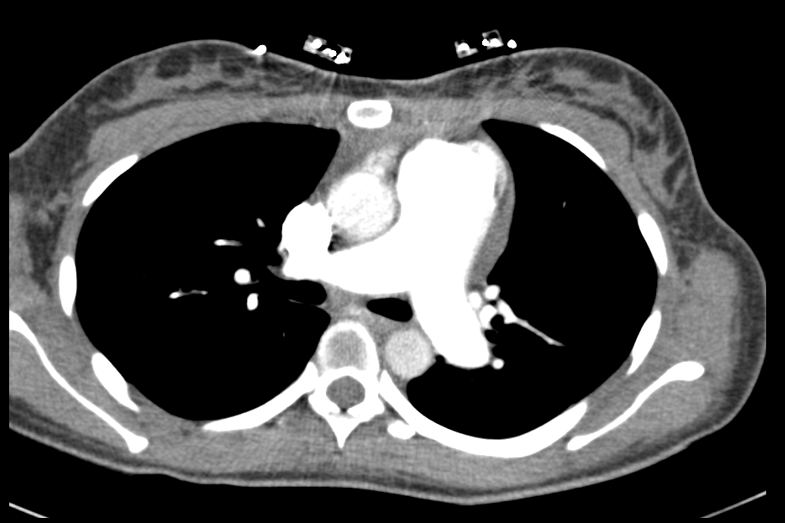
A chest CTA is appropriate for further evaluation of pulmonary artery hypertension and to rule out etiologies interstitial lung disease, COPD, pulmonary emboli, or vasculitis.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
Chest CTA
The pulmonary artery is:
The chest CTA shows an enlarged main pulmonary artery, further confirming the diagnosis of pulmonary artery hypertension.
There are lung findings to explain the cause of the pulmonary artery hypertension.
There is air trapping suggested by the scattered mosaic attenuation. However, there is no evidence of lung disorders such as interstitial lung disease, COPD, pulmonary emboli, or vasculitis, which could cause secondary pulmonary hypertension.
View the full study if you'd like to like a look yourself
Third Imaging Study
What is the next imaging study you will order?
No further imaging is required.
What is your Diagnosis now that you have seen the imaging results?
The chest CT revealed cardiomegaly and an enlarged pulmonary artery, indicative of pulmonary artery hypertension. No evidence of a lung disorder, such as interstitial lung disease, COPD, pulmonary emboli, or vasculitis, which could lead to secondary pulmonary hypertension, was found.
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
Considering the chronicity of the patient's symptoms, routine evaluation is appropriate.
Assessment and Plan
Please provide your assessment and plan for this patient
This 28-year-old female presents with worsening dyspnea on exertion. Imaging showed cardiomegaly and an enlarged pulmonary artery. The findings suggest primary or idiopathic pulmonary arterial hypertension, as no underlying lung disorder was detected. Cardiology and pulmonary should be consulted for further evaluation and management, including right heart catheterization, pulmonary function testing, and echocardiography for definitive diagnosis and assessment of disease severity. If symptoms are severe, calcium channel blockers or ACE inhibitors may be considered.
Lessons Learned:
- Idiopathic pulmonary arterial hypertension (IPAH) is a rare, progressive disease characterized by elevated pulmonary artery pressure without an identifiable cause.
- In IPAH, pulmonary vascular remodeling obstructs blood flow, increasing right ventricular afterload, leading to right-sided heart failure.
- Symptoms are non-specific and may include dyspnea on exertion, fatigue, chest pain, syncope, and edema.
- Chest X-ray may reveal cardiomegaly and enlarged pulmonary arteries, while chest CTA can further characterize these findings and help rule out an underlying cause. If secondary to lung disorders such as interstitial lung disease, COPD, pulmonary emboli, or vasculitis, it is classified as secondary pulmonary arterial hypertension.
- Right heart catheterization is the gold standard for diagnosing IPAH and assessing disease severity, showing a resting mean pulmonary artery pressure of 25 mmHg or above.
- Treatment options include pulmonary vasodilators, anticoagulants, diuretics, and oxygen therapy. In severe cases, lung transplantation may be necessary.
Socioeconomic Factors: Patients with a lower socioeconomic status are at a higher risk of death of PAH.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Next


{kind=link}
{kind=link}
{kind=link}