Retake
N2) Sudden-onset severe headache
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a patient with a headache.
- Review the DDx considerations in a patient with a headache.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating patients with a headache.
History
A 50-year-old male is brought to the ED by his daughter. The patient initially reported a sudden onset of the “worst headache of his life” one hour ago. He then developed nausea, vomiting, and progressive confusion. There is no history of trauma or falls in the last few weeks.
Physical Exam
BP: 160/92, HR 92, RR 18, Temp 100.2F, O2 saturation 98%. General: Photophobia. Neuro: Pain with passive neck flexion.
Labs
Unremarkable
Provisional Diagnosis
Select the Dx you believe is most appropriate
The sudden onset of these symptoms makes an intracranial hemorrhage most likely. The constellation of findings including a “thunderclap” headache with associated vomiting, photophobia, and neck stiffness (likely secondary to meningeal irritation from blood) makes subarachnoid hemorrhage the most likely type of subarachnoid hemorrhage.
Well done. You were correct
Potential Acuity
What is your assessment of the likely acuity for this patient?
Well done. You were correct
This patient requires emergent workup and management. Subarachnoid hemorrhage that is not promptly managed can lead to significant morbidity and mortality.
First Imaging Study
What is the first imaging study you will order?
A non-contrast head CT is the best initial imaging modality to evaluate for acute intracranial hemorrhage.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
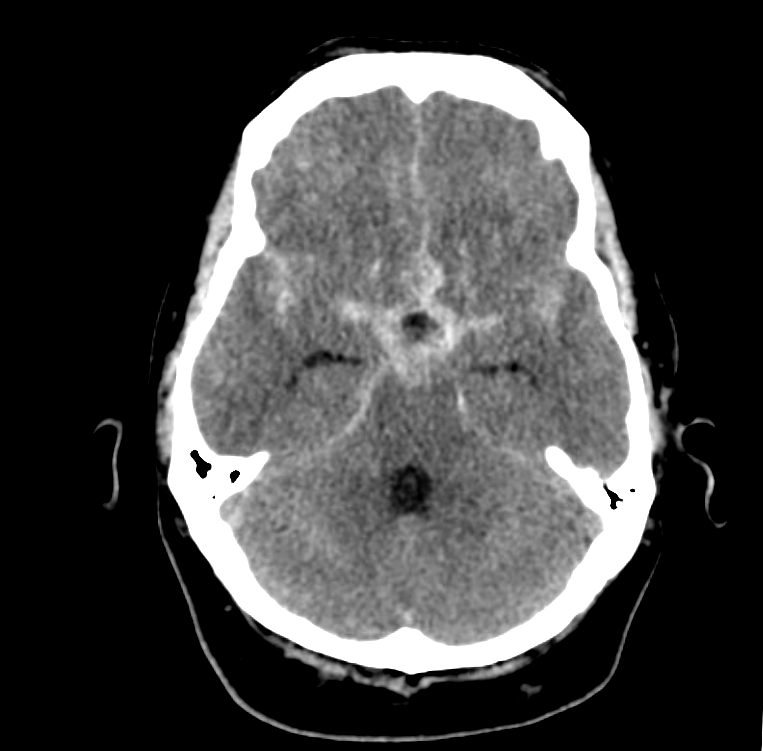
Non-Contrast CT
What best describes the findings on the Non-Contrast CT?
The fluid with high attenuation is consistent with blood. The distribution in the basal cisterns, sulci, and interhemispheric fissures is consistent with subarachnoid hemorrhage. An epidural hemorrhage appears as a lens shaped collection of blood that remains within suture lines. A subdural hemorrhage would present as a crescent shaped collection of blood that crosses suture lines.
There is intraventricular extension.
Severe subarachnoid hemorrhage can present with intraventricular extension. In this case, there is no blood in the ventricles.
There are signs of communicating hydrocephalus.
Subarachnoid hemorrhage can acutely cause noncommunicating hydrocephalus by obstructing CSF drainage pathways or may chronically cause communicating hydrocephalus by scarring arachnoid granulations. In this case, the ventricles are not dilated.
View the full study if you'd like to take a look yourself.
Second Imaging Study
What is the next imaging study you will order?
A CTA of the brain should be performed to evaluate for an aneurysm, which is the leading cause of nontraumatic subarachnoid hemorrhage.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
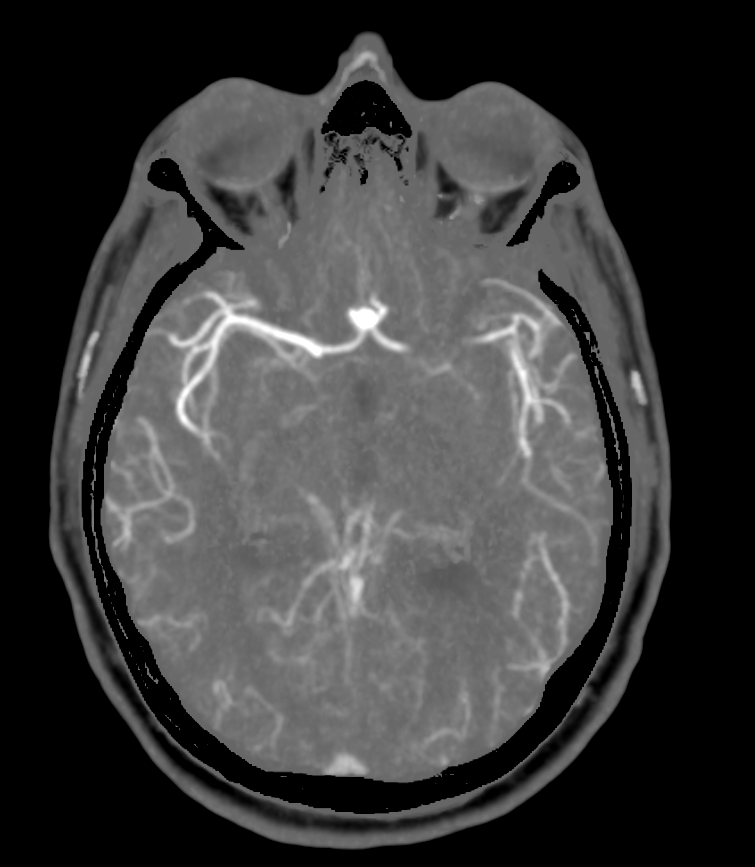
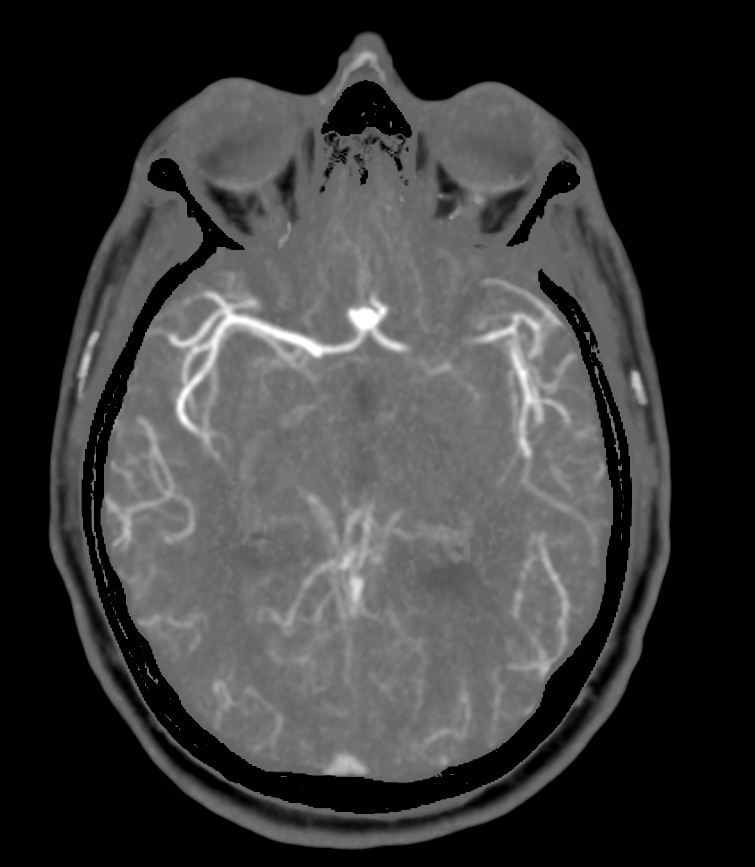
Brain CTA
There is an aneurysm on the brain CTA?
There is an aneurysm.
The aneurysm is in the:
The aneurysm occurs at the anterior communicating artery.
View the full study if you'd like to like a look yourself
What is your Diagnosis now that you have seen the imaging results?
This patient is presenting with intracranial hemorrhage. Specifically, he is presenting with a subarachnoid hemorrhage secondary to an aneurysmal rupture.
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
The patient requires emergent workup and management.
Assessment and Plan
Please provide your assessment and plan for this patient
This patient is presenting with a subarachnoid hemorrhage secondary to a rupture of an aneurysm in the anterior cerebral artery. Depending on the institution, neurosurgery or interventional neurology should be emergently consulted for evaluation for surgical clipping or endovascular coiling. The patient will also require ICU admission with frequent neurological exams. Nimodipine should be started to prevent vasospasm. The patient should be monitored, like with serial neurological examinations, for vasospasms and delayed cerebral ischemia.
Lessons Learned:
- Subarachnoid hemorrhage classically presents with a thunder-clap headache with the maximal intensity reached within one minute.
- The blood may lead to meningeal irritation and neck stiffness.
- Nontraumatic SAH are most commonly due to ruptured saccular aneurysms. These saccular aneurysms most often occur at branch points. Specifically, they often occur at the junction between the anterior cerebral artery and anterior communicating artery.
- CT scan without contrast is the preferred initial imaging study which can show acute hemorrhage (high-density signal) in the distribution of the subarachnoid space. This may be followed by a CTA to evaluate for the etiology.
- A ruptured aneurysm can be managed by surgery (craniotomy with aneurysm clipping) or endovascular methods (coiling, stenting, or combined methods) to control the bleed and prevent re-bleeding.
Socioeconomic Factors: Smoking and excessive alcohol intake are risk factors for developing cerebral aneurysms. Therefore, patients, particularly those with known aneurysms too small to benefit from intervention, should be counseled to abstain from these habits.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Next


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}