A13) Abdominal pain and bilious vomiting
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a patient with nausea and vomiting.
- Review the DDx considerations in a patient with nausea and vomiting.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating a patient with nausea and vomiting.
History
Physical Exam
Labs
Provisional Diagnosis
Potential Acuity
What is your assessment of the likely acuity for this patient?
First Imaging Study
What is the first imaging study you will order?
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
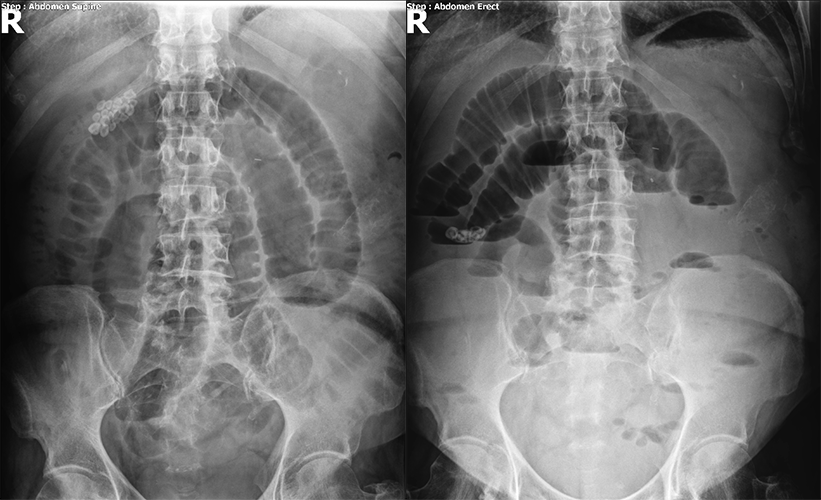
Abdominal X-ray
Which part of the intestine is dilated?
There are incidental findings.

Watch our video
Second Imaging Study
What is the next imaging study you will order?
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
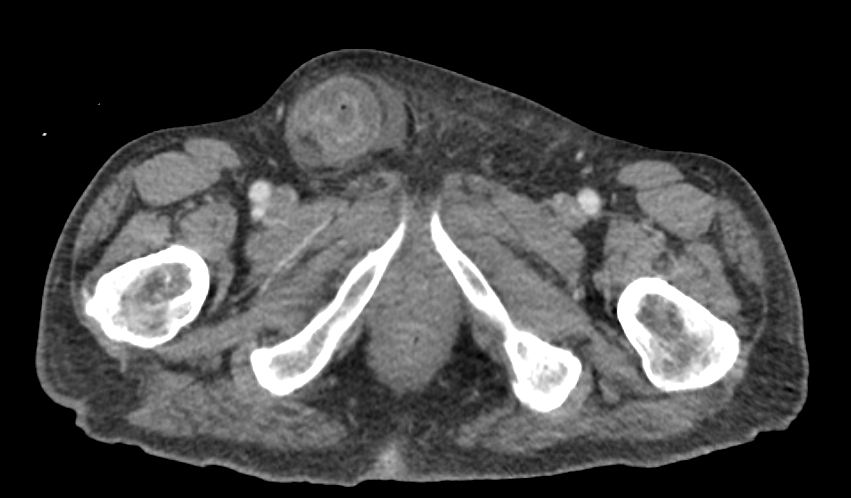
CT abdomen
There are dilated loops of small bowel.
The hernia is strangulated.
There is a transition point.
Watch our video
Third Imaging Study
What is the next imaging study you will order?
What is your Diagnosis now that you have seen the imaging results?
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
Assessment and Plan
Please provide your assessment and plan for this patient
Lessons Learned:
- Small bowel obstruction may occur secondary to post-operative abdominal adhesions, hernias, tumors, foreign bodies, volvulus, intussusception, and inflammatory or infectious processes.
- In some cases, like with bowel obstruction secondary to abdominal adhesions, patients may undergo a trial of conservative treatment with NPO, bowel decompression with a nasogastric tube, and fluid and electrolyte administration.
- Adhesions are the most common cause of small bowel obstructions in the U.S.
- A KUB may differentiate a mechanical versus adynamic ileus and assess for complications like free abdominal air.
- The cause of the small bowel obstruction can be assessed for using a CT scan.
Socioeconomic Factors: Patients with lower socioeconomic status or without private insurance are more likely to present to the emergency department with uncomplicated hernias, likely secondary to a lack of access to outpatient surgical care.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.

{kind=link}
{kind=link}
{kind=link}
{kind=link}