Retake
N25) Paralysis after trauma
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a patient with neck pain.
- Review the DDx considerations in a patient with neck pain.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating patients with neck pain.
History
A 20-year-old male is brought into the trauma bay following a high-speed motorcycle collision. He was intubated at the scene as he was initially minimally responsive. He was also unable to move his extremities. A chest X-ray confirms that the ETT is in good position.
Physical Exam
BP: 130/85, HR 115, RR 12, Temp 99F, O2 saturation 96%.
Neuro: Neck stabilized in C-collar. Sedation and paralytics are reduced to perform a neurologic examination. There is exquisite tenderness to palpation over the cervical spine. The patient cannot move his arms or legs on command. 2/5 strength in the bilateral upper extremities and 1/5 in bilateral lower extremities.
Labs
Unremarkable.
Provisional Diagnosis
Select the Dx you believe is most appropriate
The patient’s cervical spine tenderness with a palpable stepoff and associated neurologic deficits strongly suggests spinal cord injury.
Well done. You were correct
Potential Acuity
What is your assessment of the likely acuity for this patient?
Well done. You were correct
This patient with suspected spinal cord injury requires emergent workup and evaluation to maximize their chances of functional recovery.
First Imaging Study
What is the first imaging study you will order?
Patients who do not meet the NEXUS criteria should get a CT of the cervical spine without IV contrast as the initial test to evaluate for spinal trauma. While an MRI can directly assess for spinal cord injury, it is not the ideal first study as it is more time-consuming. Furthermore, a CT better assesses bone. In this setting of acute trauma, a trauma series CT scan should be obtained, which evaluates the brain, neck, chest, and abdomen. Considering that there is suspected cervical spine injury, a CTA to evaluate the neck vasculature would also be obtained. For the purposes of this case, we show the non-contrasted neck findings.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
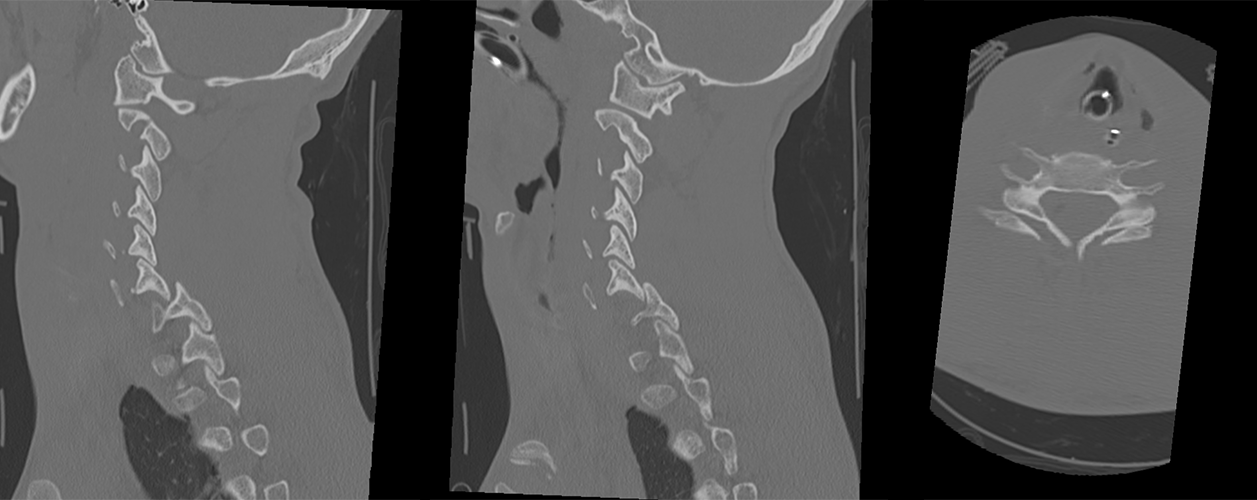
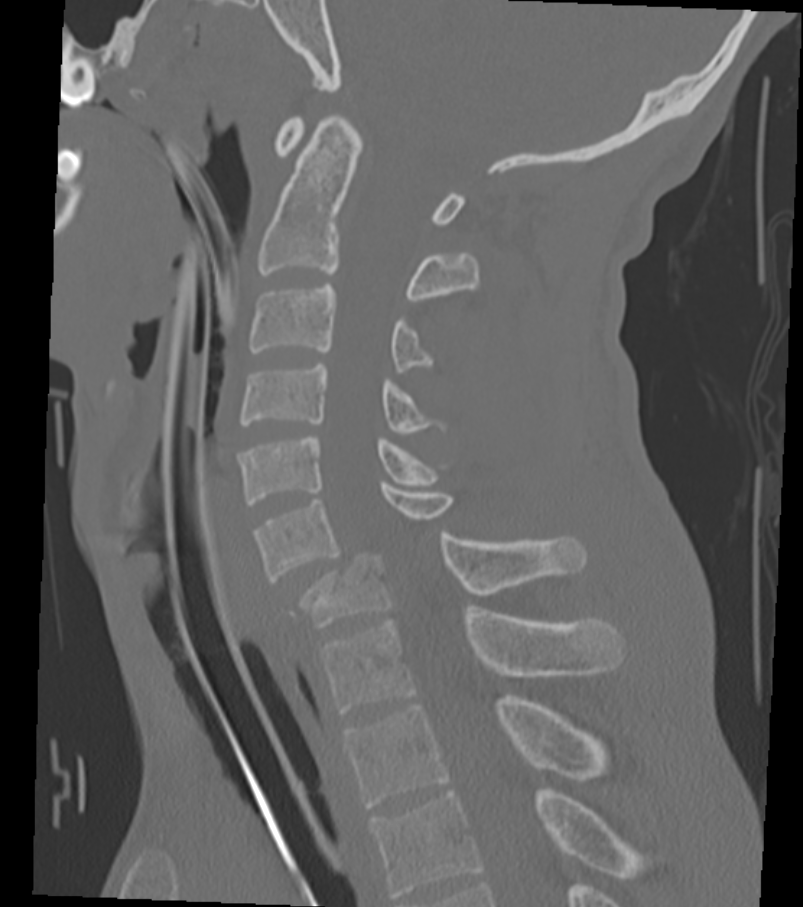
CT C-spine without contrast
The facet joints are normally aligned.
There are bilateral jumped and locked facets at C6-C7. On the sagittal view, the C7 superior articular facet is abnormally posterior to the C6 inferior articular facet. This is visible on the axial view as the “naked facet sign,” or “reverse hamburger sign.”
The spinal column demonstrates:
There is severe anterior subluxation of the C6 vertebral body over the C7 vertebral body. This results in severe traumatic cervical canal narrowing.
View the full study if you'd like to take a look yourself.
Second Imaging Study
What is the next imaging study you will order?
An MRI may be performed to evaluate for ligamentous injury, an epidural hematoma, and spinal cord injury. However, given the patient's injury pattern and CT findings, which strongly suggests spinal cord and ligamentous injury, surgical intervention without further imaging may be appropriate, as was the case with this patient.
Well done. You were correct
What is your Diagnosis now that you have seen the imaging results?
All of the above findings are present, as seen on CT scan.
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
This patient with suspected spinal cord injury requires emergent workup.
Assessment and Plan
Please provide your assessment and plan for this patient
A 20-year-old male involved in a high-speed motor vehicle collision presents with cervical spine tenderness, a palpable stepoff, and neurologic deficits. CT imaging revealed bilaterally locked facets at C6-C7, resulting in severe cervical canal stenosis with a high probability of spinal cord injury, and a C7 vertebral body fracture.
The patient requires emergent neurosurgical evaluation and should be kept in a cervical collar. IV methylprednisolone administration should be considered to reduce inflammation and attempt to minimize further spinal cord damage. The patient should also receive optimal pain control and undergo physical and occupational therapy as soon as they are stable post-operatively to maximize functional recovery.
Lessons Learned:
· When a trauma patient presents with neck pain and severe neurological deficits, such as quadriplegia or paraplegia, severe spinal cord injury should be considered as a differential diagnosis. This may be caused by fractures, dislocations, or subluxations of the spine.
· Locked facets in the cervical spine are a consequence of severe flexion injury, usually in the lower cervical spine. This condition arises when the superior articular facet of a lower vertebral level becomes "locked" posterior to the inferior articular facet of the superior vertebra. This may happen unilaterally or bilaterally.
· In over 90% of cases, bilateral locked facets in the cervical spine are associated with severe neurological deficits, often resulting in quadriplegia. Disruption of all ligamentous structures is usually present at the level of the dislocation.
· Immediate neurosurgical intervention is required in such cases, which may involve closed reduction or open reduction with fixation.
Socioeconomic Factors: In patients with this type of injury, the time to intervention is critical, as the chances of motor function recovery decrease with every passing minute. Therefore, accessibility to spine surgeons is essential for the definitive treatment of this injury.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Next


{kind=link}
{kind=link}