N23) Low back pain after a fall
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a patient with back pain.
- Review the DDx considerations in a patient with back pain.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating patients with back pain.
History
Physical Exam
Labs
Provisional Diagnosis
Potential Acuity
What is your assessment of the likely acuity for this patient?
First Imaging Study
What is the first imaging study you will order?
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
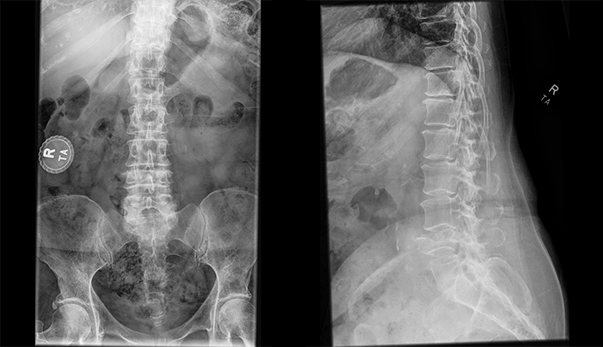
Lumbar spine radiograph
There is a vertebral body fracture at
There is an incidental finding

Watch our video
Second Imaging Study
What is the next imaging study you will order?
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
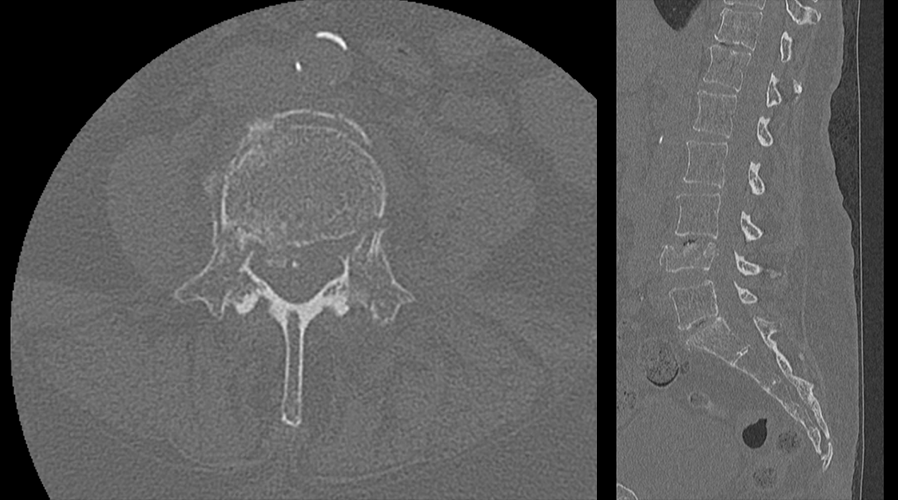
Lumbar spine CT
The fracture extends into the pedicles
There is retropulsion of the fracture fragments
Watch our video
Third Imaging Study
What is the next imaging study you will order?
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
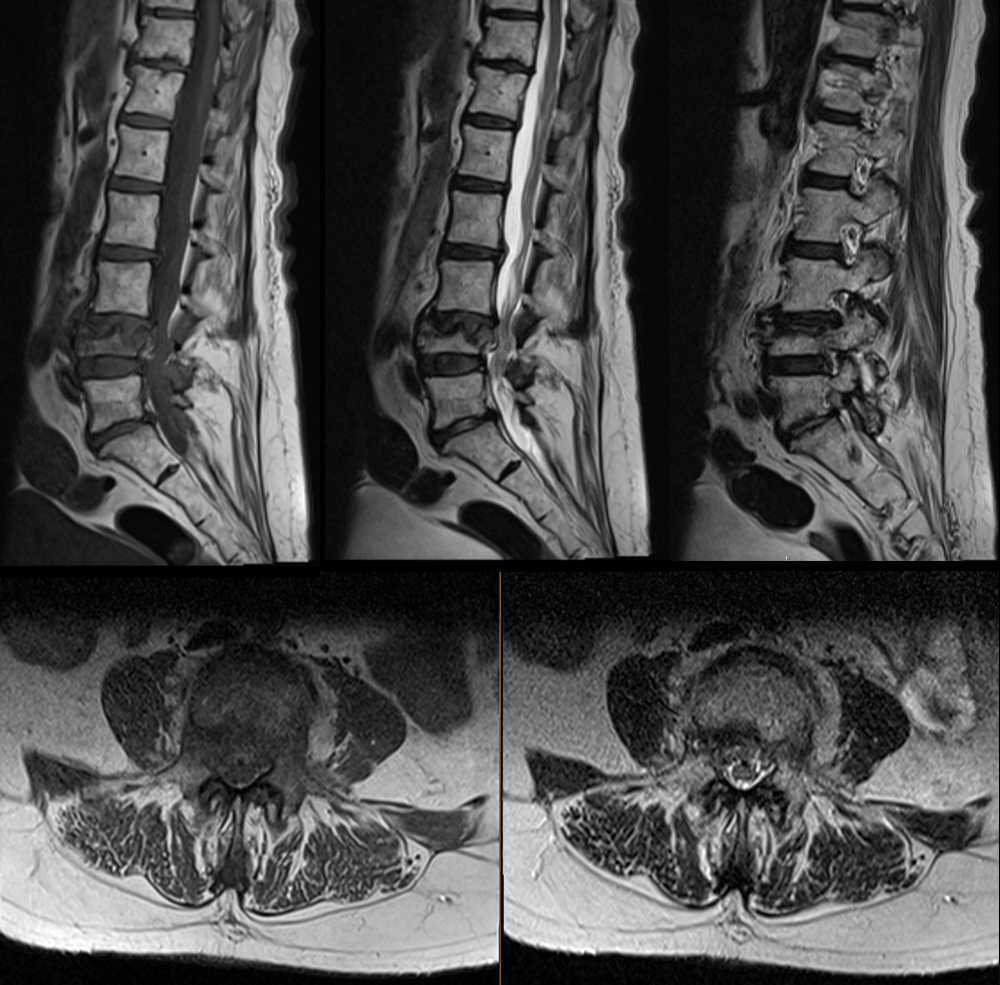
Lumbar spine MRI
There is spinal canal stenosis.
There is L4 foraminal stenosis.
Watch our video
What is your Diagnosis now that you have seen the imaging results?
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
Assessment and Plan
Please provide your assessment and plan for this patient
Lessons Learned:
- Compression fractures include wedge fractures, split fractures, and burst fractures. Burst fractures involve an endplate and the posterior cortex of the vertebral body.
- Burst fractures with retropulsed segments can result in spinal canal stenosis.
- A compression fracture is unstable when two contiguous columns are involved. The columns are as follows:
- Anterior: anterior 2/3 of vertebral body
- Middle: posterior 1/3 of vertebral body
- Posterior: pedicles and neural arch
Socioeconomic Factors: Patients with low back pain without red flags presenting for the first time should not undergo routine imaging. A focused history and physical examination should be performed. The patient should be reassured, provided with initial analgesics, and referred to physical therapy if necessary. Red flags include prolonged corticosteroid use, immunosuppression, known or suspected cancer, IV drug use, urinary tract infections, fever, pain not improved with rest, significant trauma, bladder or bowel incontinence, urinary retention, diminished anal sphincter tone, lower extremity motor weakness, point tenderness, limited range of motion of the spine, persistent neurologic findings, and saddle anesthesia.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Contributors:
Kevin Pierre, MD - Editor
Robbie Slater, MD - Supervising Editor
Bayar Batmunh, MS - Coordinator

{kind=link}
{kind=link}
{kind=link}
{kind=link}