Retake
C16) Dyspnea on exertion in a patient with history of MI
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a patient with hypoxia.
- Review the DDx considerations in a patient with hypoxia.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating a patient with hypoxia.
History
A 54-year-old male with a PMH significant for T2DM and MI 5 years ago (s/p CABG w/ double bypass) presents due to progressive shortness of breath over the last year. The patient uses more pillows at night to sleep to prevent shortness of breath. At night, he often has a nonproductive cough and awakens short of breath. He is now dyspneic with ordinary physical activities, like walking up a flight of stairs.
Physical Exam
BP: 124/90, HR 92, RR 21, Temp 36.4, O2 saturation 89%. Pulmonary: crackles and wheezing in all lung fields. 2+ pitting edema in bilateral lower extremities. GI: Liver palpable below costophrenic margin. Abdomen mildly distended, shifting dullness to percussion, positive fluid wave. CV: S3 gallop. Laterally displaced point of maximal impulse. Elevated JVP.
Labs
BNP 1,000 pg/mL
Provisional Diagnosis
Select the Dx you believe is most appropriate
The patient likely has CHF considering history of ischemic heart disease and other risk factors (T2DM, and male sex). The physical examination findings suggest CHF (cardiomegaly, S3 gallop) with both left (pulmonary edema, paroxysmal nocturnal dyspnea, orthopnea) and right (ascites, hepatomegaly, pitting edema, elevated JVP) sided involvement.
Well done. You were correct
Potential Acuity
What is your assessment of the likely acuity for this patient?
Well done. You were correct
This patient is not at risk for immediate decompensation. However, they require further workup.
First Imaging Study
What is the first imaging study you will order?
A chest x-ray may rule out other pulmonary causes of dyspnea.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
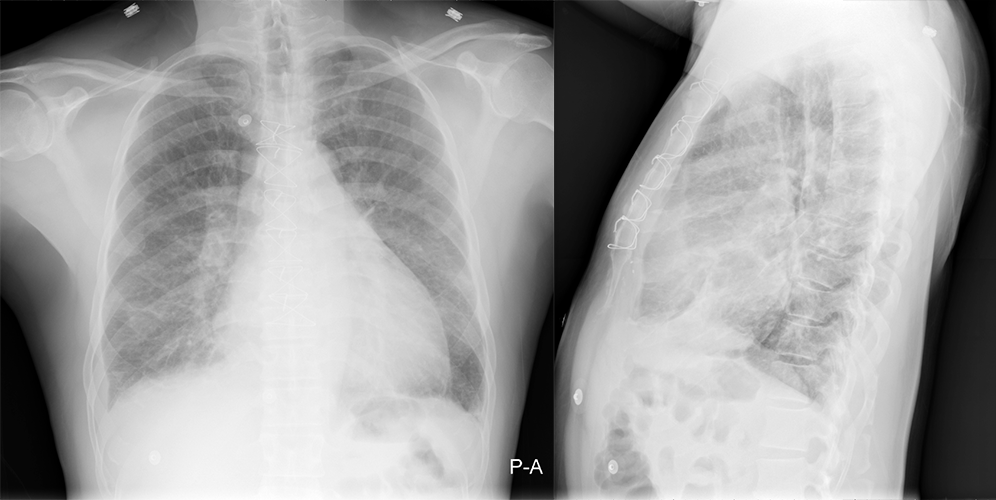
2 view chest x-ray
What best describes the findings on the Chest X-ray?
Pulmonary edema is represented by interstitial edema. Alveolar edema also occurs in more advanced cases. Fluid also leaks into the interlobular septa, appearing as “Kerley B” lines. The cardiac silhouette is enlarged secondary to cardiomegaly. The increased left atrial pressure leads to pulmonary vascular congestion and cephalization of the pulmonary veins. Note that there is peribronchial cuffing from fluid leaking into the peribronchial interstitium. These findings are consistent with CHF.
There is pulmonary edema.
There is interstitial edema. Fluid also leaks into the interlobular septa, appearing as “Kerley B” lines. The increased left atrial pressure leads to pulmonary vascular congestion and cephalization of the pulmonary veins. There is also peribronchial cuffing from fluid leaking into the peribronchial interstitium. Taken together, these findings represent pulmonary edema. In the setting of cardiomegaly, the diagnosis is most consistent with CHF.
View the full study if you'd like to take a look yourself.
Second Imaging Study
What is the next imaging study you will order?
The current clinical picture is highly consistent with CHF. Chest CT is unlikely to provide any additional helpful information.
Well done. You were correct
What is your Diagnosis now that you have seen the imaging results?
Once the diagnosis is confirmed, the patient would be classified into NYHA II CHF as they have symptoms with ordinary physical activities. (NYHA I: no symptoms; III: symptoms during less than ordinary physical activity, IV: symptoms at rest.)
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
This patient is not at risk for immediate decompensation but requires further workup.
Assessment and Plan
Please provide your assessment and plan for this patient
54-year-old male presenting with signs, symptoms, labs, and imaging consistent with CHF. An echocardiogram will be obtained and cardiology will be consulted. A diuretic trial will be administered. The patient will benefit from further laboratory workup to rule out comorbidities and contributing etiologies.
Lessons Learned:
- Chest x-ray findings for CHF include (1) cardiomegaly (2) pulmonary vascular congestion and cephalization of the pulmonary veins, (3) pulmonary edema (interstitial edema and later alveolar edema; Kerley B lines; peribronchial cuffing, (4) and pleural effusions.
Socioeconomic Factors: Patients who may not closely follow up with their PCP should be counseled extensively on their disease and the required dietary and lifestyle modifications prior to discharge.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Next


{kind=link}