Retake
V1) Sudden onset leg pain in a patient with atrial fibrillation
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a patient with lower extremity pain.
- Review the DDx considerations in a patient with lower extremity pain.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating a patient with lower extremity pain.
History
A 35-year-old male with past medical history of a hyperlipidemia, uncontrolled diabetes mellitus, myocardial infarction 2 years ago, and atrial fibrillation with poor medication compliance presents due to new onset severe right lower extremity pain and parasthesias.
Physical Exam
BP: 122/79, HR 104, RR 18, Temp 36.8, O2 saturation 100%. Extremities: RLE: cool to touch, pale, and tender to palpation. No audible arterial doppler signal or palpable pulse in DP, PT, or popliteal arteries. Venous signals are present. Reduced ability to dorsiflex and plantar flex right foot. Severe pain in leg when dorsiflexing and plantar flexing right foot. Right lower leg appears enlarged and is tense compared to left. Cardiovascular: fast rate and irregular rhythm. Neuro: minimal sensory impairment throughout right lower extremity including forefoot.
Labs
Unremarkable.
Provisional Diagnosis
Select the Dx you believe is most appropriate
The most likely diagnosis is acute limb ischemia. The patient presents with the characteristic “P”s – poikilothermia, pain, pallor, pulselessness, paresthesias, and paralysis. In this case, it is likely secondary to a cardiac embolus considering the atrial fibrillation, history of myocardial infarction, and acute onset.
Well done. You were correct
Potential Acuity
What is your assessment of the likely acuity for this patient?
Well done. You were correct
This condition is immediately limb-threatening and therefore requires emergent evaluation.
First Imaging Study
What is the first imaging study you will order?
A CTA of the lower extremities can evaluate the vasculature of the lower extremities for the presence of acute limb ischemia and if present, allow for surgical planning.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
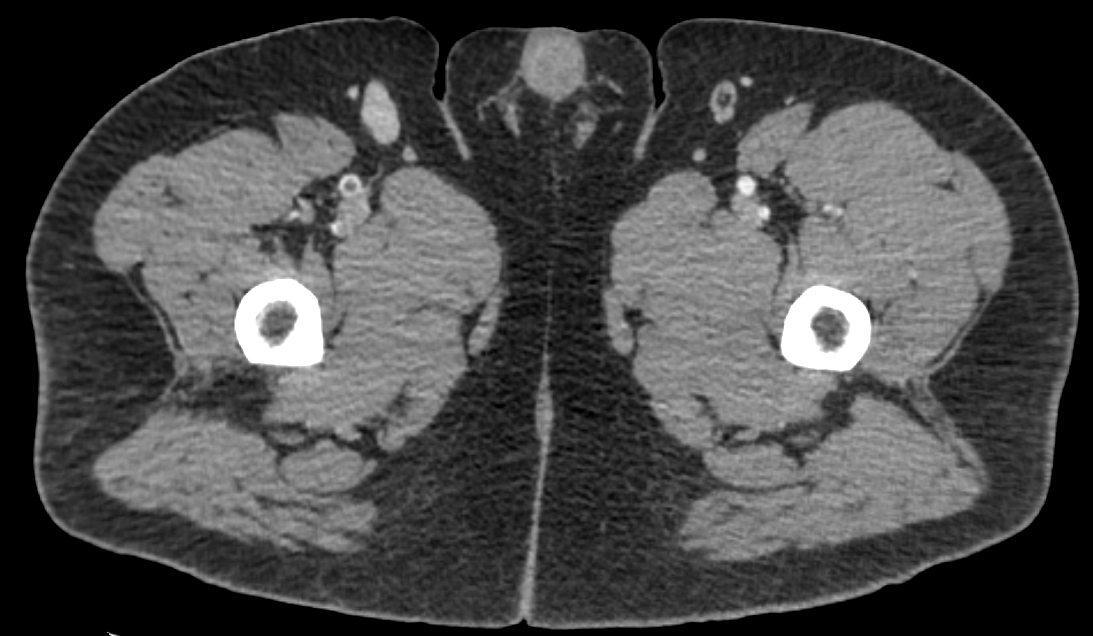
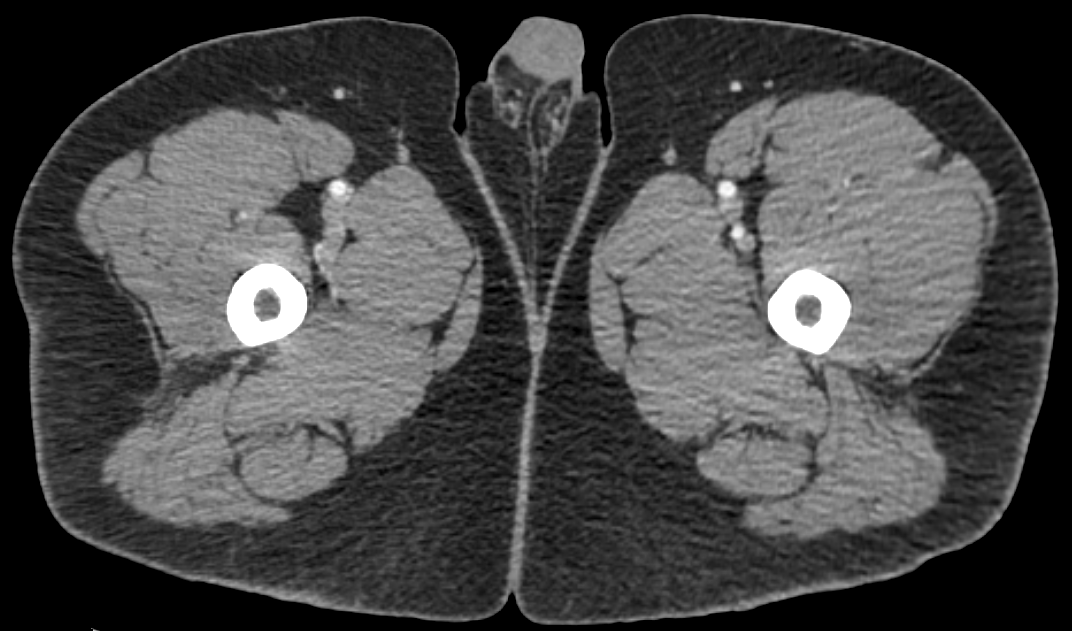
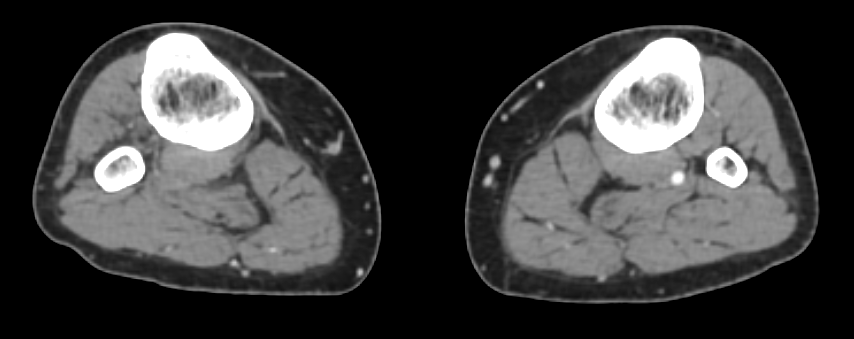
CTA abdomen and pelvis with leg runoff
There is a thrombus in the right popliteal artery.
There is a thrombus in the right popliteal artery causing complete occlusion.
View the full study if you'd like to take a look yourself.
Second Imaging Study
What is the next imaging study you will order?
None. The diagnosis is confirmed using CTA.
Well done. You were correct
What is your Diagnosis now that you have seen the imaging results?
The patient has class Rutherford class 2b acute limb ischemia considering the acute onset leg pain with motor and sensory impairment and absent arterial doppler signals. Therefore, the limb is immediately threatened. (Class 1: no impairment with present signals; no immediate threat to limb. Class 2a: minimal sensory impairment with present signals; marginally threatened limb. Class 3: absent arterial and venous pulses with insensate leg and rigorous motor impairment; irreversible ischemia requiring amputation).
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
The patient will require emergent vascular intervention.
Assessment and Plan
Please provide your assessment and plan for this patient
This patient is a 35-year-old male presenting with Rutherford class IIb acute limb ischemia and compartment syndrome likely secondary to thrombus from uncontrolled afib. Vascular surgery should be immediately consulted to evaluate for revascularization and fasciotomy as their limb is immediately threatened. Following intervention, an echocardiogram and hypercoagulable workup can be performed. The patient will also require management and counseling for their uncontrolled atrial fibrillation and diabetes.
Lessons Learned:
- Acute limb ischemia should be suspected in patients presenting with acute onset leg pain with characteristic signs and symptoms.
- CTA or catheter-guided angiography are good initial tests in confirming the diagnosis.
- Evaluation and management should be considered emergent in Rutherford class IIb ischemia considering that the limb is at immediately threatened.
Socioeconomic Factors: Patients with lower socioeconomic status with acute limb ischemia have higher readmission rates and present with more severe comorbidities compared to those with higher socioeconomic status.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Contributors:
Kevin Pierre, MD - Editor
Robbie Slater, MD - Supervising Editor
Bayar Batmunh, MS - Coordinator
Next


{kind=link}
{kind=link}
{kind=link}