R1) Abdominal pain and vaginal bleeding in a patient who missed her menstrual cycle
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a patient with abdominal pain and vaginal bleeding.
- Review the DDx considerations in a patient with abdominal pain and vaginal bleeding.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating patients with abdominal pain and vaginal bleeding.
History
Physical Exam
Labs
Provisional Diagnosis
Potential Acuity
What is your assessment of the likely acuity for this patient?
First Imaging Study
What is the first imaging study you will order?
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
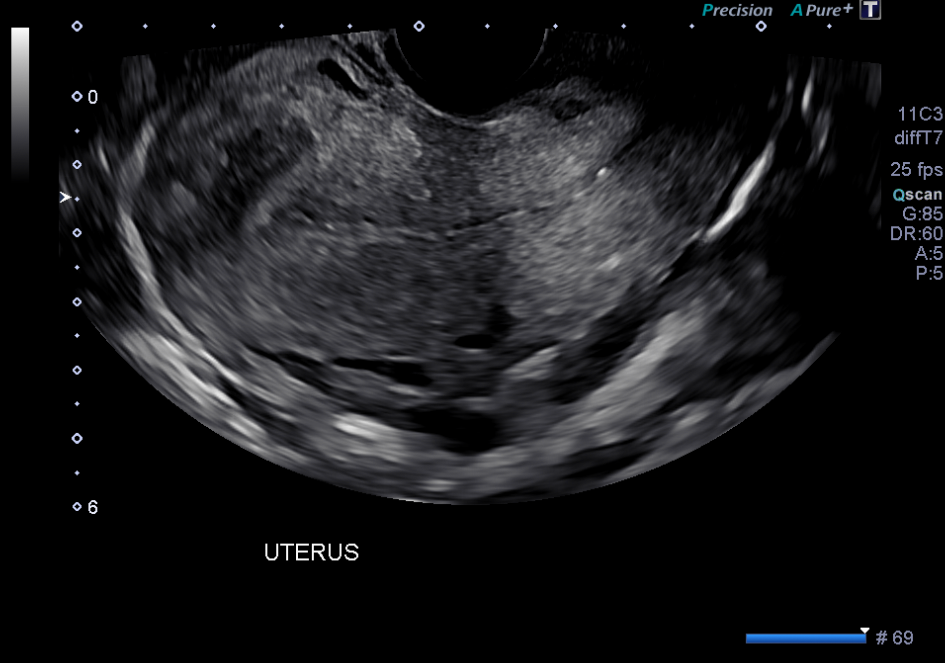
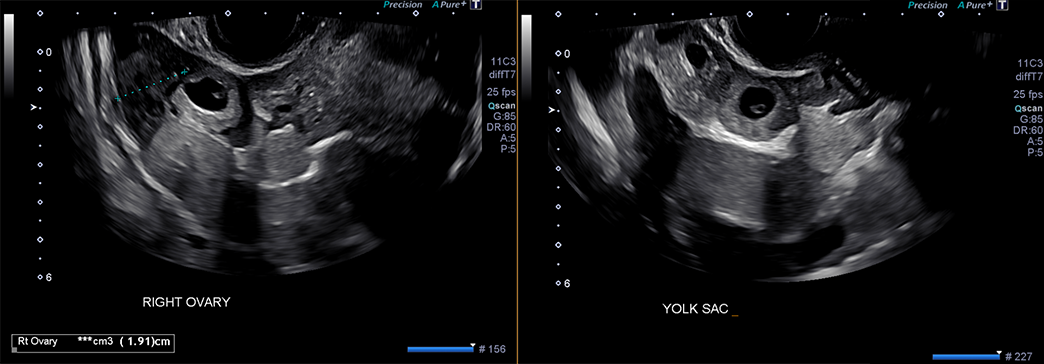
Abdominal ultrasound
There is a gestational sac located in the uterus.
There is a gestational sac located in the right adnexa.

Watch our video
Second Imaging Study
What is the next imaging study you will order?
What is your Diagnosis now that you have seen the imaging results?
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
Assessment and Plan
Please provide your assessment and plan for this patient
Lessons Learned:
- Ectopic pregnancy is more likely to occur in older patients of childbearing age. Other risk factors include prior ectopic pregnancy, endometriosis, IVF treatment, certain STI’s, pelvic inflammatory disease, tubal surgery, and presence of an IUD.
- The diagnosis should be suspected in a patient with positive pregnancy test, vaginal bleeding, and lower abdominal pain. These findings are certainly nonspecific and occur in other conditions, including IUP. However, ectopic pregnancy is a “cannot miss” diagnosis.
- Transvaginal ultrasound is the imaging modality of choice and should be used to evaluate uterine and adnexal anatomy to assess for presence of ectopic pregnancy. An extrauterine gestational sac or echogenic heterogenous mass confirms the diagnosis when paired with physical exam, presentation, and lab findings.
Socioeconomic Factors:
- Ectopic pregnancy and related death are persistently higher in African American women and other racial/ethnic minorities.
- Women from all racial/ethnic minority groups were significantly more likely than white women to experience at least one complication during treatment, such as the need for a blood transfusion, and were more likely to experience a longer hospitalization.
- Among those with ectopic pregnancy who required surgical intervention, uninsured women have less frequently undergone tubal conserving surgery (salpingostomy).
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Contributors:
Thomas Kent, MS2 - Content Contributor
Alexandria Hotop - Content Contributor
Kevin Pierre, MD - Editor
Robbie Slater, MD - Supervising Editor
Bayar Batmunh, MS - Coordinator

{kind=link}
{kind=link}