Retake
N7) Weakness and parasthesias in an immunosuppressed patient
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a patient with weakness.
- Review the DDx considerations in a patient with weakness.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating a patient with weakness.
History
A 55-year-old male with a history of end-stage renal disease (ESRD) underwent a kidney transplant six months ago. He has been maintained on immunosuppressant medications since then. He was recently admitted due to Nocardial pneumonia and daily falls at home, with symptoms present for about 2-3 weeks. The patient has been experiencing right-sided weakness, intermittent paresthesias in the upper and lower extremity, and daily falls, usually to the left side. His weakness, numbness, and tingling have significantly improved since being started on antibiotics. He has a history of COPD that is managed with bronchodilators and corticosteroids.
Physical Exam
BP: 120/83, HR 102, RR 20, Temp 102F, O2 saturation 97%.
HEENT: Pupils are equal round and reactive to light.
Cardiopulmonary exam: Normal.
Neurological Exam: Cranial nerve examination is grossly intact. Motor strength is normal in all extremities. Mild dysmetria, dysdiadochokinesia, and intention tremors are noted on finger-nose-finger testing.
Labs
Complete Blood Count (CBC):
White Blood Cell count (WBC): 15,000 cells/mm³ (Reference range: 4,500-11,000 cells/mm³).
Inflammatory Markers:
C-reactive Protein (CRP): 25 mg/L (Reference range: <5 mg/L);
Erythrocyte Sedimentation Rate (ESR): 50 mm/h (Reference range: 0-20 mm/h for men).
Blood Cultures:
Pending results.
Provisional Diagnosis
Select the Dx you believe is most appropriate
Considering the patient's history of immunosuppression, recent pneumonia, current fever, elevated white blood cell count and inflammatory markers, as well as the improvement of neurological symptoms after antibiotic treatment, the patient is likely suffering from multiple brain abscesses resulting from septic emboli from the lungs.
Well done. You were correct
Potential Acuity
What is your assessment of the likely acuity for this patient?
Well done. You were correct
The patient requires urgent workup and management.
First Imaging Study
What is the first imaging study you will order?
The best initial imaging modality for a suspected brain abscess is an MRI of the head. In this patient with "red flags" including fever, neurologic deficits, history of immunocompromise, and older age (>50 years), an MRI an appropriate initial imaging modality. It provides detailed and sensitive evaluation of the brain.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
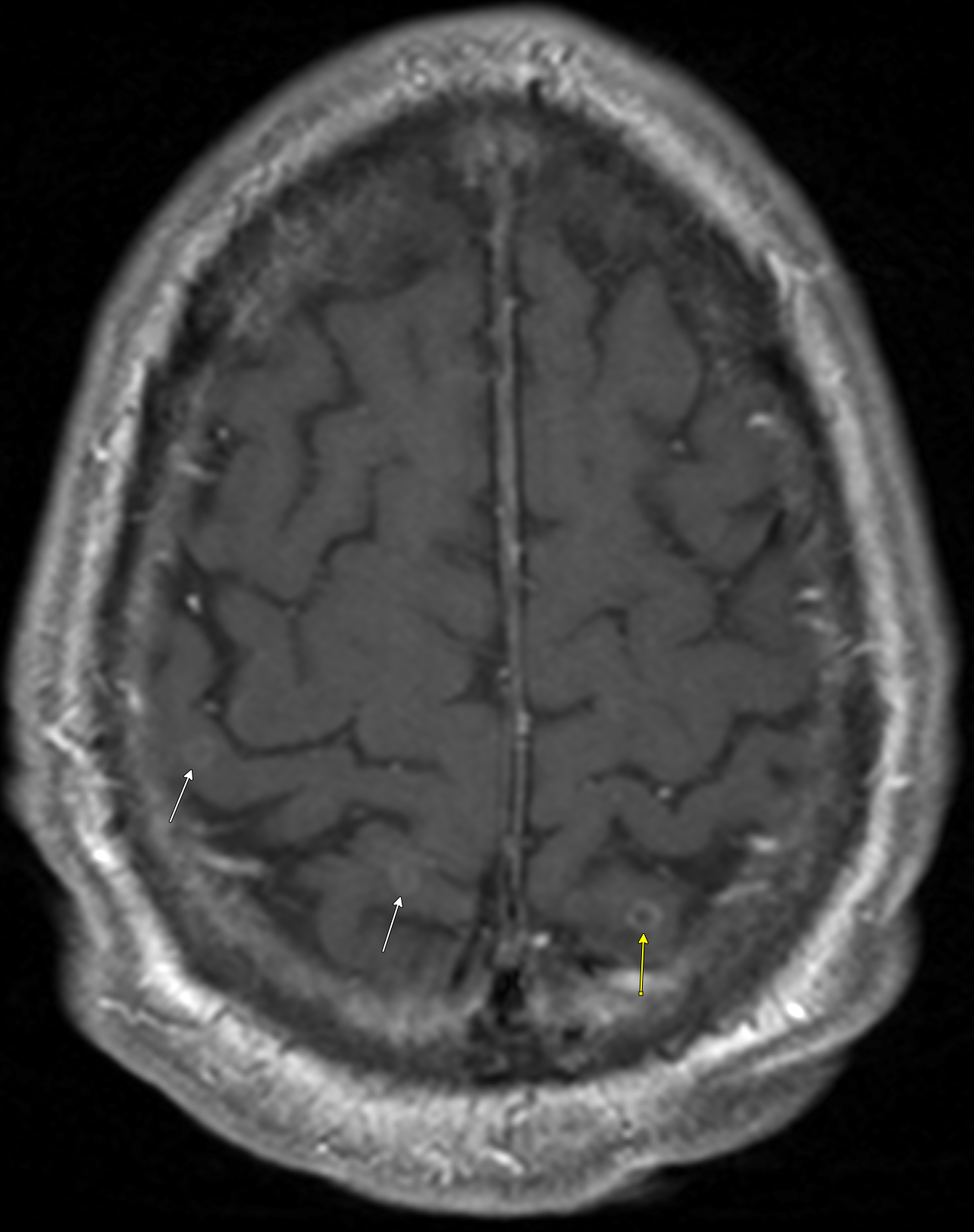
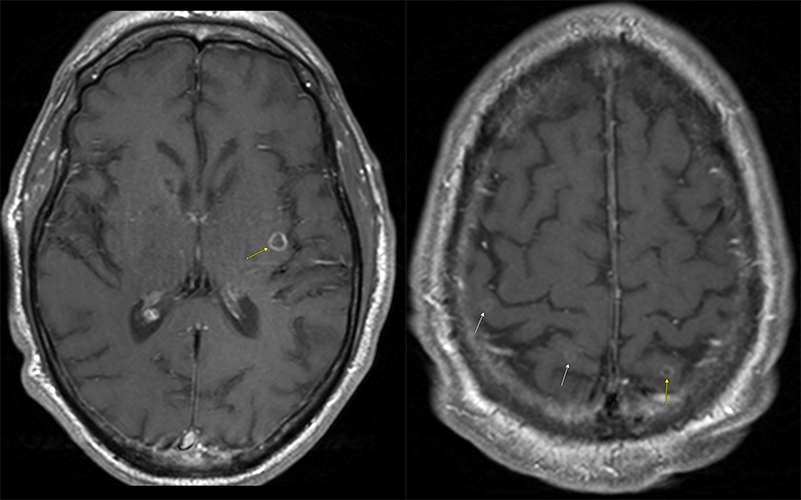
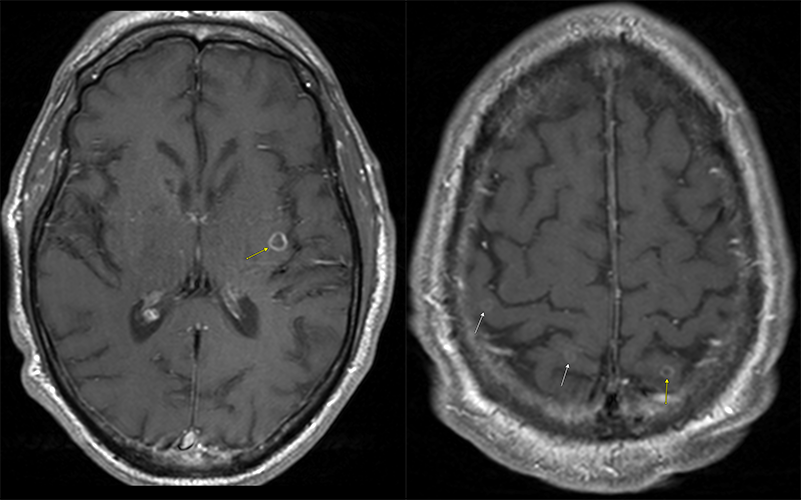
MRI Head
The brain lesion is in the:
The lesion is in the left insular cortex.
How many brain lesions are present?
There are multiple brain lesions present.
What are the characteristics of the lesion walls?
The lesion walls are thin, regular, and enhancing, which are consistent with abscesses. In contrast, a glioblastoma often exhibits thick, nodular, enhancing walls.
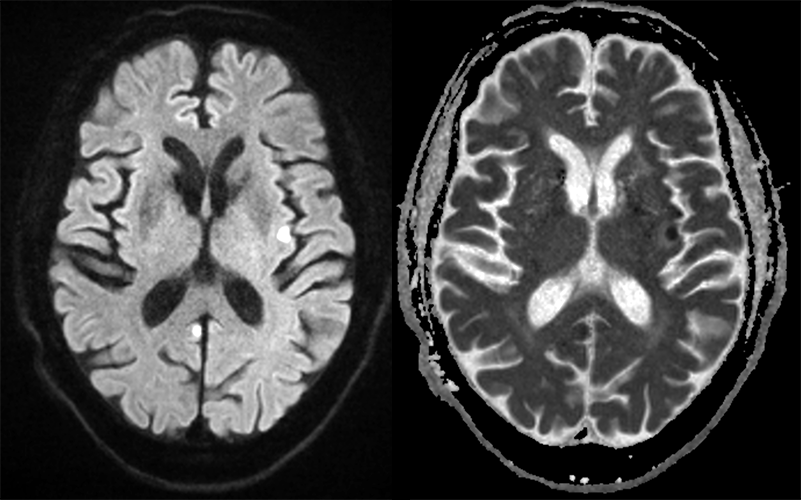
Does the lesion demonstrate diffusion restriction?
The lesion demonstrates diffusion restriction, as it appears bright on the trace sequence and dark on the ADC.
View the full study if you'd like to take a look yourself.
Second Imaging Study
What is the next imaging study you will order?
A CTA of the head and neck could be considered to evaluate for mycotic aneurysms as a potential cause of the septic emboli. However, given the patient's known Nocardial pneumonia, this is less likely.
Well done. You were correct
What is your Diagnosis now that you have seen the imaging results?
In this patient, it is most likely that the brain abscesses have developed as a result of septic emboli originating from the Nocardial pneumonia.
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
The patient requires a routine, but expedited workup, as the lesions are small, non-compressive, and the patient's symptoms are already improving with treatment for Nocardial pneumonia.
Assessment and Plan
Please provide your assessment and plan for this patient
The 55-year-old male patient, who is on immunosuppressive medications following a kidney transplant, has recently experienced neurological deficits while being treated for Nocardial pneumonia. Imaging studies reveal multiple small, non-compressive, peripherally enhancing lesions throughout the cerebrum, indicative of brain abscesses. Although a CTA of the head and neck could evaluate for mycotic aneurysms as a potential cause of septic emboli, it is less likely due to the patient's known Nocardial pneumonia. Given the improvement in symptoms with ongoing treatment, Nocardial brain abscesses are the most likely diagnosis. The patient should continue targeted antibiotic therapy with an antibiotic like trimethoprim-sulfamethoxazole (TMP-SMX) as a first-line lipophilic antibiotic that crosses the blood-brain-barrier, with adjustments based on sensitivity testing, and consider. Regular follow-ups, including serial MRI scans, are essential for monitoring the patient's progress.
Lessons Learned:
- CNS Nocardiosis, a rare bacterial infection primarily affecting immunocompromised individuals, often manifests as multiple small brain abscesses.
- Brain abscesses due to Nocardiosis typically arise as septic emboli resulting from pulmonary Nocardiosis dissemination, with patients initially presenting with pulmonary symptoms. Therefore, this diagnosis should be suspected in immunocompromised patients with known lung disease presenting with brain abscesses. However, some patients may present with primary brain lesions.
- Notable subtypes that spread to the brain include Nocardia beijingensis, farcinica, and asteroides, among others.
- Patients can present with single or multiple abscesses, generally characterized by thin, regular, enhancing walls, diffusion restriction, and significant perilesional edema.
- While the diagnosis of CNS Nocardiosis can often be made presumptively, neurosurgical biopsy might be necessary in some cases. Minimally invasive techniques are increasingly employed to ensure patient safety.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Next


{kind=link}
{kind=link}
{kind=link}
{kind=link}