Retake
N33) Lower extremity weakness and incontinence
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a patient with weakness.
- Review the DDx considerations in a patient with weakness.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating patients with weakness.
History
A 20-year-old male presents to the neurology outpatient clinic with a one-week history of progressive sensory disturbances and lower extremity weakness. He reports a vague sensation of tightness around his chest and numbness of tingling in his legs with decreased perception of temperature changes. He also endorses new onset urinary urgency and occasional incontinence. He denies any trauma.
Physical Exam
BP: 132/84, HR 92, RR 20, Temp 98F, O2 saturation 97%. 3+ reflexes in the bilateral lower extremities with a positive Babinski’s sign bilaterally. Wide-based, unsteady gait. Decreased pinprick, temperature, and vibration sensation below the T1 dermatome.
Labs
None
Provisional Diagnosis
Select the Dx you believe is most appropriate
The patient’s onset of bilateral lower extremity motor and sensory deficits with urinary symptoms, their progression, the positive Babinski sign bilaterally, and the absence of pain or trauma history make transverse myelitis a more likely diagnosis. Disc herniation or spinal canal stenosis would usually present with localized pain or radiculopathy, and the symptoms might not be as symmetric or extensive as in this case.
Well done. You were correct
Potential Acuity
What is your assessment of the likely acuity for this patient?
Well done. You were correct
The patient requires urgent workup and evaluation.
First Imaging Study
What is the first imaging study you will order?
An MRI of the spine should be ordered to assess for inflammation, demyelination, or lesions in the spinal cord. The use of contrast will enable the assessment of active inflammatory lesions and differentiate acute lesions from chronic ones.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
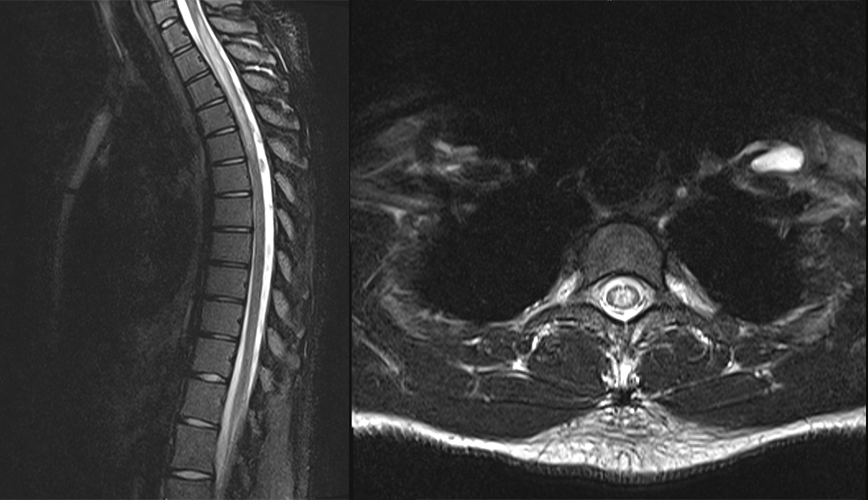
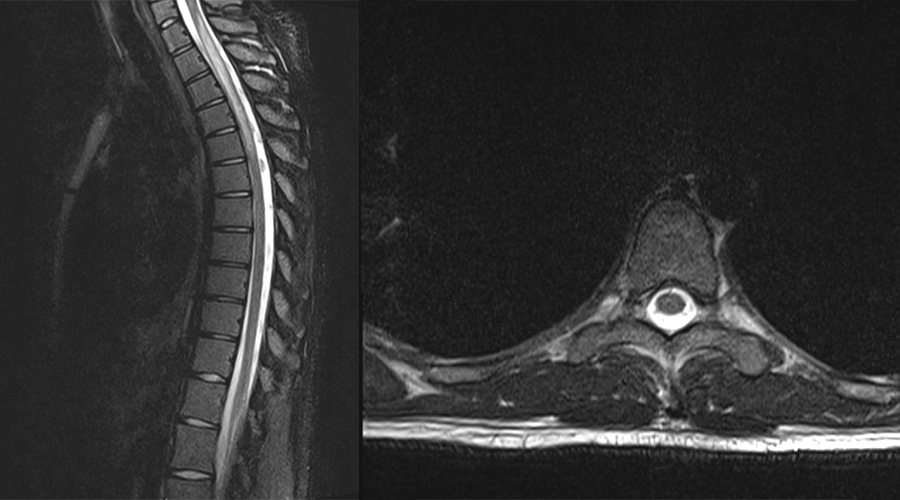
MRI spine
There is an abnormality in the cervical spine.
There are hyperintense regions within the spinal cord on the T2-weighted images, suggesting demyelination.
There is an abnormality in the lower thoracic spine.
There are no signal changes or areas of abnormal enhancement in the lumbar spine.
View the full study if you'd like to take a look yourself.
Second Imaging Study
What is the next imaging study you will order?
An MRI of the brain can be considered to rule out other conditions like multiple sclerosis, or neuromyelitis optica, which can both initially present with transverse myelitis. We do not show these images in this case as they were negative.
Well done. You were correct
What is your Diagnosis now that you have seen the imaging results?
The patient’s presentation and imaging findings are consistent with a diagnosis of transverse myelitis.
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
The patient requires urgent workup and management.
Assessment and Plan
Please provide your assessment and plan for this patient
This is a 20-year-old male patient presenting with progressive bilateral lower extremity weakness, sensory disturbances below the T1 level, and urinary urgency and incontinence. The patient's imaging findings reveal a longitudinally extensive demyelinating lesion extending from T1 to T5, suggesting a diagnosis of transverse myelitis. An MRI of the brain should be considered to rule out other conditions such as multiple sclerosis or neuromyelitis optica. The patient should be initiated on high-dose IV corticosteroids and referred to outpatient rehabilitation and a neurologist.
Lessons Learned:
- Transverse myelitis is a rare myelopathy, with fewer than 5 cases per million, potentially appearing idiopathically as in this case. It has a bimodal age distribution, occurring primarily in ages 10-20 years and 30-40 years.
- Symptoms can include spasticity, hyperreflexia, motor and sensory dysfunction, neurogenic bladder, and reproductive issues. Symptoms typically peak from 4 hours to 21 days after onset.
- An MRI typically reveals hyperintense areas, suggestive of inflammatory myelopathy. Enhancing lesions suggest active demyelination.
- Cerebrospinal fluid (CSF) analysis often shows the presence of inflammatory markers.
- High-dose IV corticosteroids remain the first-line treatment for transverse myelitis, supplemented by supportive treatment and, where appropriate, rehabilitation.
Socioeconomic Factors: Obesity has been linked to an increased likelihood of developing transverse myelitis.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Next


{kind=link}
{kind=link}