Retake
N26) Low back pain and fever in a patient with history of IV drug use
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a patient with back pain.
- Review the DDx considerations in a patient with back pain.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating patients with back pain.
History
A 57-year-old male with a history of IV drug use presents to the ED with fever and severe lower back pain. The pain began approximately 6 weeks ago and initially improved with bed rest. It has progressively worsened and is now constant. He now notes pain radiating to his abdomen, groin, and lower extremities. More recently, he has difficulty walking with numbness and tingling in both legs. He denies any history of spinal injury, spinal surgery, or degenerative spinal disease.
Physical Exam
BP: 110/70, HR 110, RR 18, Temp 38C, O2 saturation 100%. General: Patient appears in distress. Musculoskeletal: Midline point tenderness over lumbar spine. Abdominal: Bladder is distended. Pain with hip extension bilaterally. Neuro: No reflexes elicited on right knee and ankle. Fasciculations present in bilateral lower extremities. Decreased rectal tone. No bulbocarvernosus reflex. There is saddle anesthesia. Skin: Needle tracks present in bilateral cubital fossae and between fingers.
Labs
Total leukocyte count: 21 x 10^9/L (nl range 4.5-11 x 10^9/L); Absolute neutrophil count: 10,100 (nl range 2,500-6,000); Erythrocyte sedimentation rate: 120 mm/h (nl range 0-15mm/h); C-reactive protein: 12 mg/L (nl <10mg/L)
Provisional Diagnosis
Select the Dx you believe is most appropriate
This patient with a history of IV drug use with spinal point tenderness, leukocytosis, elevated ESR, and CRP likely has osteomyelitis. The distended bladder and lower motor neuron signs (fasciculation and weak reflexes) can be due to nerve root compression from an epidural abscess. The patient’s positive psoas sign suggests a psoas abscess as a complication of osteomyelitis.
Well done. You were correct
Potential Acuity
What is your assessment of the likely acuity for this patient?
Well done. You were correct
This patient’s requires emergent workup considering the new onset of neurological deficits.
First Imaging Study
What is the first imaging study you will order?
An AP and lateral X-ray of the lumbar spine should be ordered to evaluate for bony pathology.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
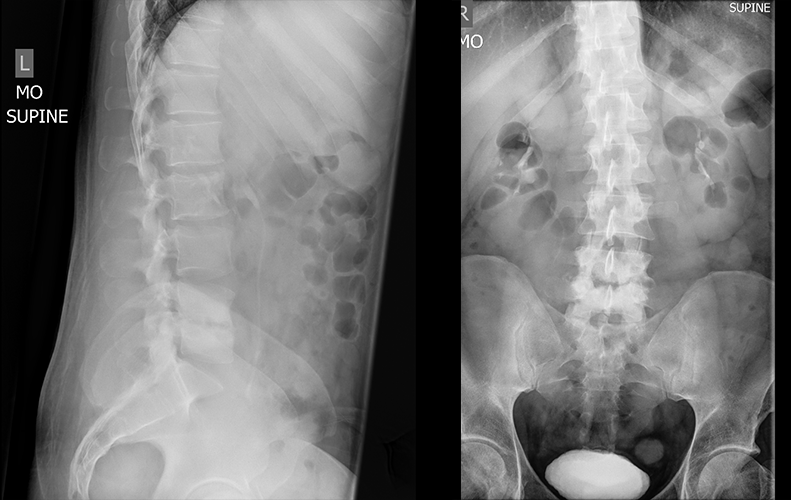
AP and lateral X-ray of the lumbar spine
There is an L4 vertebral fracture.
There is no evidence of fracture at any vertebral level.
There are erosive changes in the endplates of L4-L5 disc space.
There are extensive erosive and destructive changes on the lower end plate of L4 and upper end plate of L5.
View the full study if you'd like to take a look yourself.
Second Imaging Study
What is the next imaging study you will order?
A spine MRI can confirm the diagnosis of osteomyelitis. It can also evaluate for its complications, like an epidural abscess.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
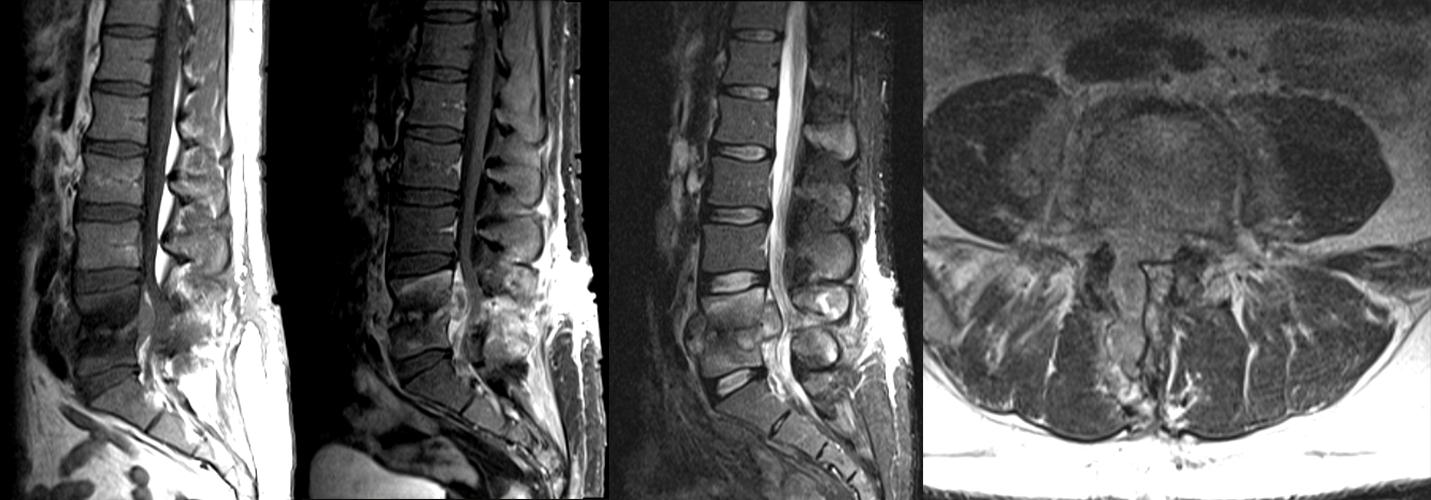
MR
There are erosive changes
There is decreased signal intensity within L4-L5 on T1 weighted imaging and increased signal intensity on T2 weighted imaging, indicative of bone marrow edema from the erosive changes.
There is an epidural abscess present that is compressing the cauda equina.
The T1 weighted images show epidural lesion with peripheral contrast enhancement, which is consistent with an abscess.
View the full study if you'd like to like a look yourself
Third Imaging Study
What is the next imaging study you will order?
No further imaging is needed as the MRI has confirmed the diagnosis of lumbar osteomyelitis discitis.
What is your Diagnosis now that you have seen the imaging results?
This patient has cauda equina syndrome secondary to osteomyelitis discitis and the mass effect of the epidural abscess on the nerve roots of cauda equina. The clinical exam with predominantly lower motor neuron symptoms with saddle anesthesia, decreased rectal tone, absent bulbocavernosus and deep tendon reflexes, and fasciculations suggest that the patient is presenting with cauda equina syndrome and not conus medullaris syndrome.
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
The patient is at risk for impending paralysis due to the spinal epidural abscess compressing the nerve roots. He therefore requires emergent workup and management.
Assessment and Plan
Please provide your assessment and plan for this patient
This patient is a 57-year-old male with a history of IV drug use, presenting with cauda equina syndrome secondary to osteomyelitis discitis of L4-L5 with epidural and psoas abscesses. The patient requires emergent neurosurgical evaluation for drainage and decompression. In the interim, blood cultures should be obtained to determine the causal organism. The patient should also be started on empirical antibiotic therapy.
Lessons Learned:
- IV drug use is a risk factor for osteomyelitis. Other risk factors include infective endocarditis, degenerative spinal disease, previous spinal surgery, diabetes, and immunocompromised status.
- Complications of osteomyelitis include spinal epidural abscesses and psoas abscesses. Spinal epidural abscesses can present with neurologic deficits and require emergent management to prevent paralysis.
Staphylococcus aureus is the most common causative agent of osteomyelitis.
- Antimicrobial treatment is administered for a minimum of 6 weeks. During this time, the patient needs to be closely monitored for clinical improvement.
- Microorganisms most commonly cause osteomyelitis through hematogenous spread. This often leads to two adjacent vertebrae being affected as arteries supplying the vertebrae bifurcate to supply two adjacent endplates.
- X-rays may look normal in the early phases of osteomyelitis. Erosive changes in X-ray indicate that the infection is advanced.
- MRI is the most sensitive imaging modality to evaluate for osteomyelitis. It can also be used to determine if the infection has spread to soft tissues.
- Spinal epidural abscesses can be visualized in MRI. Ring enhancement, as compared to heterogeneous enhancement, suggests that it is an abscess and not a phlegmon. Large abscesses can lead to spinal canal stenosis.
Socioeconomic Factors:
- Treatment for osteomyelitis requires prolonged use of expensive antibiotic treatment, lengthy hospital stays, and surgery. This proves to be a financial burden, especially for those with lower socioeconomic status.
- It is reasonable to first obtain an MRI in a patient presenting with neurologic deficits with suspected osteomyelitis to evaluate for cord compression.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Contributors:
Seyedeh Mehrsa Sadat Razavi, MS2 - Content Contributor
Kevin Pierre, MD - Editor
Robbie Slater, MD - Supervising Editor
Bayar Batmunh, MS - Coordinator
Next


{kind=link}
{kind=link}