Retake
N20) Sore throat, fever, and drooling in a child
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a patient with sore throat and fever.
- Review the DDx considerations in a patient with sore throat and fever.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating a patient with sore throat and fever.
History
A 2-year-old male presents to the emergency department accompanied by his mother. The patient's mother reports that he had four days of worsening fever, sore throat, drooling, and difficulty swallowing food due to pain. The patient is up-to-date on his vaccinations. There is no concern from the patient’s family regarding foreign body ingestion.
Physical Exam
BP: 85/65, HR 115, RR 30, Temp 102F, O2 saturation 96% on room air. General: Uncomfortable and lethargic. HENT: Posterior pharyngeal erythema and fullness. The tonsils are not enlarged. Swollen and tender cervical lymph nodes. Uvula midline. Pulmonary: Lungs are clear to auscultation. However, the patient is in mild respiratory distress.
Labs
WBC: 23,000/μL; normal range: 6,000-19,000/μL.
Neutrophils: 82%; normal range: 30-50%.
CRP: 72 mg/L (elevated).
ESR: 50 mm/hr (elevated).
Rapid strep test: Pending.
Influenza swab: negative.
Mono swab: negative.
Provisional Diagnosis
Select the Dx you believe is most appropriate
The provisional diagnosis for this 2-year-old male patient is a retropharyngeal abscess. This is supported by the clinical presentation of difficulty swallowing, high fever, fullness in the posterior pharynx, an elevated white blood cell count and elevated inflammatory markers. A peritonsillar abscess is unlikely considering the normal tonsils and midline uvula. While epiglottitis has overlapping symptoms, patients are generally older, with a “hot potato” voice, in “tripod positioning” to try to maintain their airway, and with a visible erythematous epiglottis.
Well done. You were correct
Potential Acuity
What is your assessment of the likely acuity for this patient?
Well done. You were correct
This patient requires urgent workup and management as they are at risk for airway compromise.
First Imaging Study
What is the first imaging study you will order?
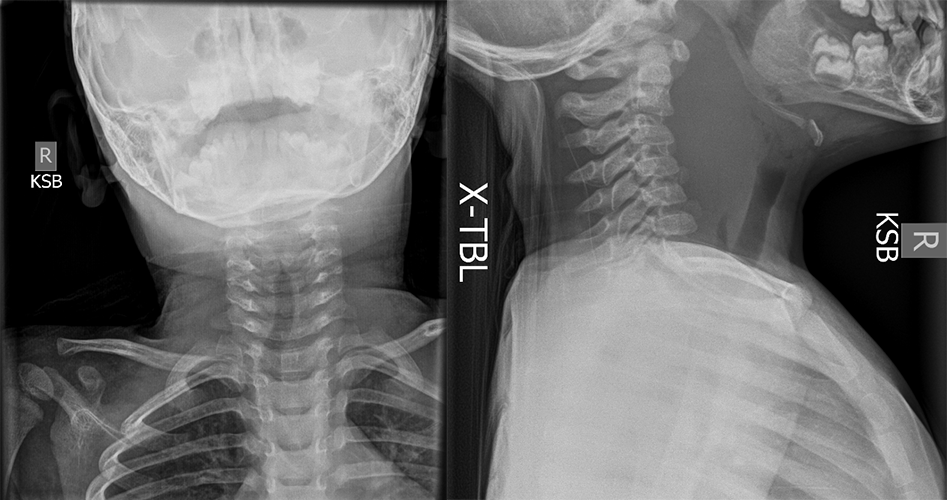
A lateral neck X-ray can be performed rapidly and can evaluate the soft tissues of the neck.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
Soft tissue neck XR
What best describes the findings on the soft tissue XR of neck?
There is widening of the soft tissue X-ray, suggestive of a retropharyngeal abscess or retropharyngeal cellulitis.
View the full study if you'd like to take a look yourself.
Second Imaging Study
What is the next imaging study you will order?
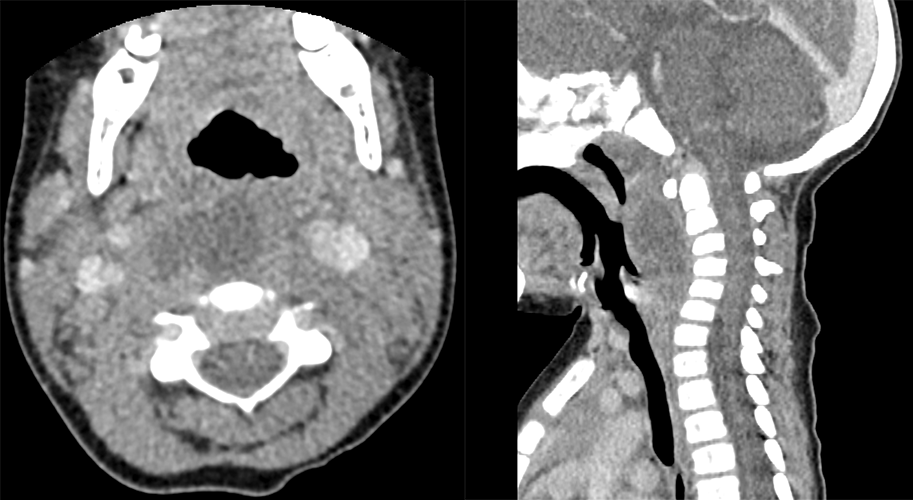
Computed tomography (CT) of the neck with intravenous contrast is the next best modality to differentiate between abscesses and cellulitis in the retropharyngeal area.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
CT Neck
In the retropharyngeal space, there is a(n):
A phlegmon is a diffuse, non-capsulated inflammatory process. It can progress to an abscess, which is a well-circumscribed collection of pus, if untreated. The findings of peripheral enhancement (representing vascularity) with a low-density center (representing a pus collection) suggests that this is an abscess. In some cases, abscesses have gas, but it is not seen in this case.
View the full study if you'd like to like a look yourself
Third Imaging Study
What is the next imaging study you will order?
No further imaging is needed.
What is your Diagnosis now that you have seen the imaging results?
The patients’ clinical presentation and imaging findings are consistent with a retropharyngeal abscess.
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
This patient needs urgent workup and management.
Assessment and Plan
Please provide your assessment and plan for this patient
A 2-year-old male presents with worsening fever, sore throat, drooling, difficulty swallowing, leukocytosis, and elevated inflammatory markers. Imaging studies confirm the presence of a retropharyngeal abscess. The patient will be admitted to the pediatric ICU. A pediatric otolaryngologist should be consulted to consider surgical drainage. In the meantime, the patient should undergo close airway monitoring and receive IV fluids and empiric IV antibiotics, which can be adjusted based on culture and sensitivity results.
Lessons Learned:
- Retropharyngeal abscesses are more common in children between the ages of two and four, but can occur at any age.
- Approximately half of retropharyngeal abscesses are thought to result from antecedent upper respiratory tract infections, while another quarter are attributed to retropharyngeal trauma.
- Imaging studies such as neck X-rays and CT scans with IV contrast can help diagnose retropharyngeal abscesses.
- A neck X-ray can reveal significant prevertebral soft tissue thickening, while a CT scan with IV contrast can provide further detail, such as a large peripherally enhancing collection in the retropharyngeal space.
- It is important to differentiate between phlegmon and abscess in the retropharyngeal space.
- A phlegmon is a diffuse, non-capsulated inflammatory process that can progress to an abscess if untreated, while an abscess is a well-circumscribed collection of pus.
- Peripheral enhancement, a low-density center, and gas on imaging suggest the presence of an abscess.
- A patient with a mature abscess with complete rim enhancement and scalloping presenting with respiratory distress and “tripod” positioning should undergo emergent surgical drainage.
Socioeconomic Factors: Hospitalization for younger children with MRSA is longer, and they are more likely to require surgery and intubation.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Next


{kind=link}
{kind=link}