Retake
C2) Fever and Cough in a Patient with Recent Stroke
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a patient with fever and cough.
- Review the DDx considerations in fever and cough.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating patients with fever and cough.
History
A 98-year-old male with a history 60-pack-year smoking history, diabetes mellitus, hypertension, and atrial fibrillation presented four days ago with a left lateral medullary ischemic stroke. Residual deficits included a hoarse voice and left sided ptosis and miosis. Yesterday, he developed a worsening productive cough with foul smelling sputum. This morning, he developed progressive altered mental status and hypoxia. A rapid response was called and he was intubated, mechanically ventilated, and transferred to the ICU. Central venous access was obtained with a PICC.
Physical Exam
BP: 105/78, HR 108, RR 22, Temp 38.9C O2 saturation 94%. General: Patient intubated. Right PICC in place. Pulmonary: Decreased breath sounds in right lower lung field.
Labs
WBC: 16 x 10^9/L.
Provisional Diagnosis
Select the Dx you believe is most appropriate
The patient has Wallenberg syndrome considering the left lateral medullary ischemic stroke with resultant left sided Horner syndrome and hoarse voice. Therefore, we should be concerned that the patient has developed aspiration pneumonia secondary to dysphagia, which is also present in Wallenberg syndrome.
Well done. You were correct
Potential Acuity
What is your assessment of the likely acuity for this patient?
Well done. You were correct
The patient requires further workup for a cause of their acute respiratory distress.
First Imaging Study
What is the first imaging study you will order?
A chest x-ray is the best first imaging study as it can be obtained quickly, can indicate the presence of pneumonia, and can rule out other life-threatening pathologies. The chest x-ray will also confirm appropriate endotracheal tube and PICC placement. The X-ray can also detect a pneumothorax, a known PICC line placement complication.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
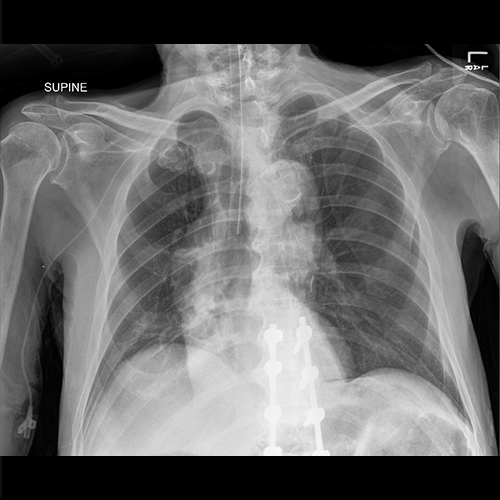
AP Chest X-ray
What best describes the findings on the AP Chest X-ray?
There is a non-specific fluffy infiltrate in the right lower lung field. The endotracheal tube is at the level of carina. The ETT should be 3cm above the carina and therefore should be retracted by 3cm.
View the full study if you'd like to take a look yourself.
Second Imaging Study
What is the next imaging study you will order?
Considering the high clinical suspicion, a CT chest can be ordered to confirm the presence of aspiration pneumonia.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
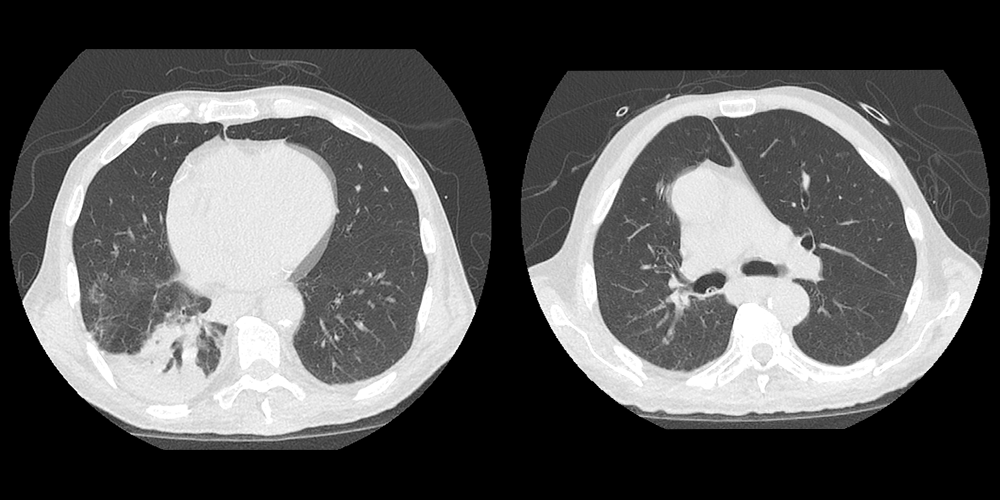
CT Chest – No IV Contrast
What best describes the findings on the CT Scan?
The patient has a consolidation in the dependent portion of the right lower lobe. There is also endobronchial debris in the right main bronchus. This is most consistent with aspiration pneumonia, which is more likely to affect the right lower lobe considering the more vertical course and larger caliber of the right main bronchus. A diagnosis of pulmonary embolism cannot be done with the current study considering the lack of IV contrast.
View the full study if you'd like to like a look yourself
What is your Diagnosis now that you have seen the imaging results?
The patient’s respiratory decompensation was most likely secondary to their aspiration pneumonia.
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
The patient has aspiration pneumonia and requires urgent further workup and treatment.
Assessment and Plan
Please provide your assessment and plan for this patient
The patient has respiratory distress secondary to aspiration pneumonia. We will obtain blood cultures and sputum cultures via deep tracheal suctioning and administer broad spectrum antibiotics with gram negative and anaerobic coverage. The antibiotics will be narrowed once the cultures result. Once the patient improves clinically, their swallow function should be evaluated by a speech therapist who can recommend dietary modifications to avoid future aspiration events. Their bed should also remain elevated.
Lessons Learned:
1) There should be a high clinical suspicion for aspiration pneumonia in patients with posterior circulation strokes.
2) Aspiration pneumonia often appears on imaging in the dependent portion of the right lower lobe considering the vertical course and larger caliber of the right main bronchus compared to the left main bronchus. Generally, they occur in the basilar portions of bilateral lower lobes in upright patients. In supine patients, often appear in the posterior segments of the upper lobes and the superior segments of the lower lobes.
Socioeconomic Factors: Risk factors for aspiration pneumonia include dementia, altered mental status, older age, and impaired swallow function. As such, they often occur in patients in nursing homes. Other risk factors include general anesthesia induction, dysphagia, GERD, CNS disorders, and TBI.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Contributors:
Kevin Pierre, MD - Editor
Robbie Slater, MD - Supervising Editor
Next


{kind=link}
{kind=link}