Retake
C9) Chest-wall pain after an ATV accident
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a patient with an incidental finding.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating patients with incidental findings.
History
A 39-year-old female presents to the ED following an ATV accident. She was able to ambulate following the accident but complains of left posterior chest wall pain, worsened with deep breaths. She denies any smoking, drugs, or alcohol.
Physical Exam
BP: 125/70, HR 72, RR 19, Temp 36.2C, O2 saturation 99%. Pulmonary: Lungs clear to auscultation bilaterally. CV: Normal S1/S2, no murmurs, rubs, or gallops, normal rate and regular rhythm. Skin: Left chest wall ecchymosis with minimal tenderness to palpation.
Labs
None
Provisional Diagnosis
Select the Dx you believe is most appropriate
The above diagnoses are all possible. However, the unremarkable physical exam findings make rib fractures and a pneumothorax less likely.
Well done. You were correct
Potential Acuity
What is your assessment of the likely acuity for this patient?
Well done. You were correct
The patient requires routine, but expedited workup to rule out pathologies like a pneumothorax secondary to rib fractures. This is not urgent, however, as she is hemodynamically stable and without physical exam findings suggesting a pneumothorax.
First Imaging Study
What is the first imaging study you will order?
A chest X-ray may identify rib fractures, pneumothorax, and traumatic aortic injury.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
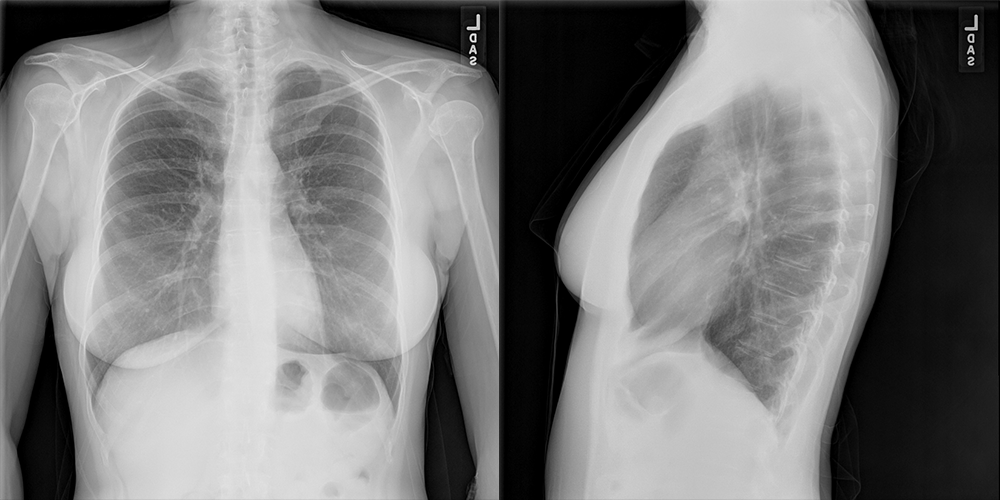
PA and Lateral Chest X-ray
What best describes the findings on the Chest X-ray?
There is a lung nodule overlying the right mid-lung. There are no rib fractures, pneumothorax, or widened mediastinum.
View the full study if you'd like to take a look yourself.
Second Imaging Study
What is the next imaging study you will order?
A chest CT can characterize this nodule and grossly assess its malignancy risk. It can also evaluate for other nodules or adenopathy that are not seen in the X-rays.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
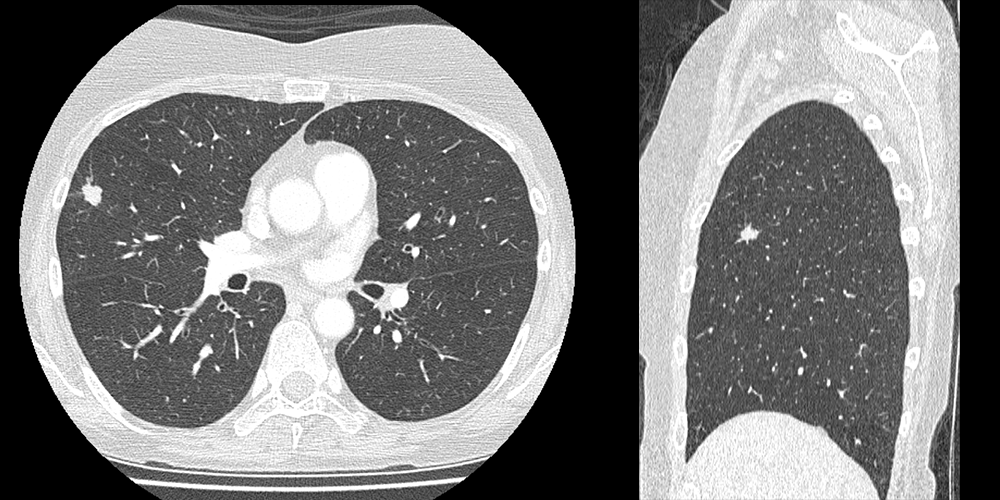
Chest CT
What best describes the findings on the Chest CT?
There is a nodule in the right middle lobe with spiculated margins. Identification of the lobe is easiest on the sagittal view.
View the full study if you'd like to like a look yourself
Third Imaging Study
What is the next imaging study you will order?
A PET CT can evaluate for tumor radiotracer uptake, nodal involvement, and metastases.
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
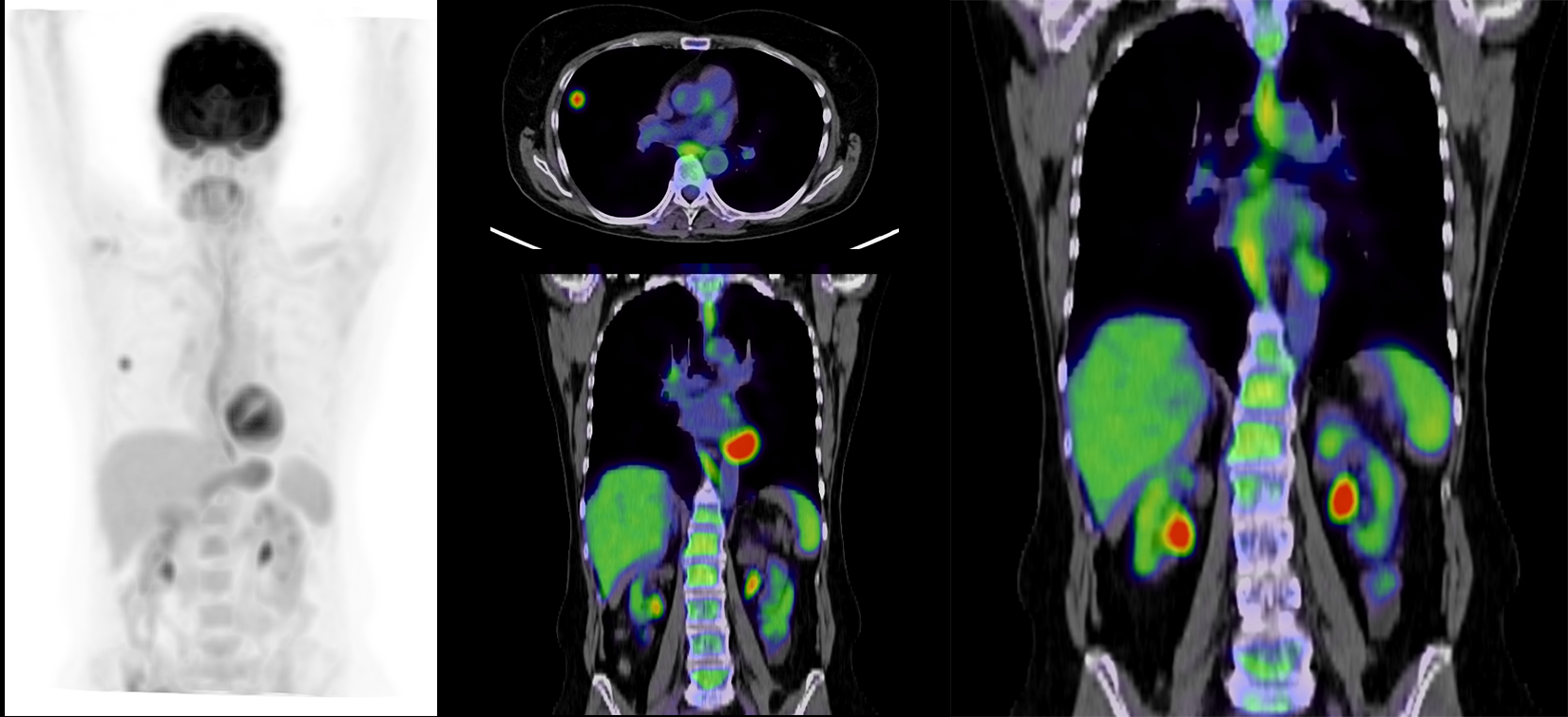
PET CT
What best describes the findings on the PET CT?
There is increased FDG uptake in the right hilum and right middle lobe lesion. The FDG in the bilateral renal hila represent physiologic excretion.
What is your Diagnosis now that you have seen the imaging results?
This lesion is unlikely a benign nodule like a hamartoma considering the spiculated margins. Squamous cell lung cancer is characteristically central. Small cell lung cancer is usually diffuse when diagnosed as it metastasizes early. This young patient without smoking history who is presenting with a peripheral lung nodule most likely has an adenocarcinoma.
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
While this condition is not immediately life threatening, this patient requires further workup.
Assessment and Plan
Please provide your assessment and plan for this patient
This is a 39-year-old female without smoking history presenting with a peripheral lung nodule with spiculated borders. This is likely an adenocarcinoma. The patient should be referred to a pulmonologist. She may undergo PET CT and endobronchial ultrasound for further characterization. If the lesion is confirmed to be a T1N0M0 (no nodal involvement or metastases), this patient may require a lobectomy with radiological surveillance.
Lessons Learned: Lung adenocarcinomas are the most common cancer in young females, non-smokers, patients under 40, and in the peripheral lung. Lung masses with poorly defined, spiculated borders are likely malignant.
Socioeconomic Factors: All imaging should be carefully evaluated for incidental findings regardless of the indication. Early detection of malignancy may significantly reduce morbidity and mortality.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Contributors:
Kevin Pierre, MD - Editor
Robbie Slater, MD - Supervising Editor
Bayar Batmunh, MS - Coordinator
Next


{kind=link}
{kind=link}
{kind=link}