Retake
A8) Flank pain and hematuria
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a patient with flank pain.
- Review DDx considerations in a patient with flank pain.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating a patient with flank pain.
History
A 25-year-old female with a history of hyperparathyroidism and celiac disease presents for worsening severe right flank pain that radiates to the groin. The pain is sharp and intermittent, lasting up to 30 minutes. She also endorses bloody urine, nausea, and vomiting.
Physical Exam
BP: 129/79, HR 98, RR 18, Temp 36.4C, O2 saturation 100%. Abdominal exam: Significant right costovertebral angle tenderness.
Labs
Urinalysis: Urine bloody in color. 15RBC/hpf on microscopy. CMP: creatinine: 1.5 (baseline 0.8 at PCP visit)
Provisional Diagnosis
Select the Dx you believe is most appropriate
The colicky flank pain radiating to the groin, with costovertebral angle tenderness suggests renal colic from obstruction of the ureter. In this young patient with a history of hyperparathyroidism (results in hypercalciuria) and celiac disease (results in hyperoxaluria), it is likely secondary to a kidney stone.
Well done. You were correct
Potential Acuity
What is your assessment of the likely acuity for this patient?
Well done. You were correct
Considering the patient has acute kidney injury (Cr >1.5x baseline), they require expedited workup.
First Imaging Study
What is the first imaging study you will order?
An abdominal CT without contrast is the gold standard for identifying and characterizing renal stones. The pelvis should also be included to assess for stones in the lower ureter, ureterovesical junction, and the bladder.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
CT abdomen and pelvis without contrast
The kidney stone is at the
The stone is at the junction between the renal pelvis and ureter, one of the three common stone entrapment areas secondary to anatomical narrowing of the ureter.
There is hydronephrosis
There is hydronephrosis secondary to the obstructing stone.
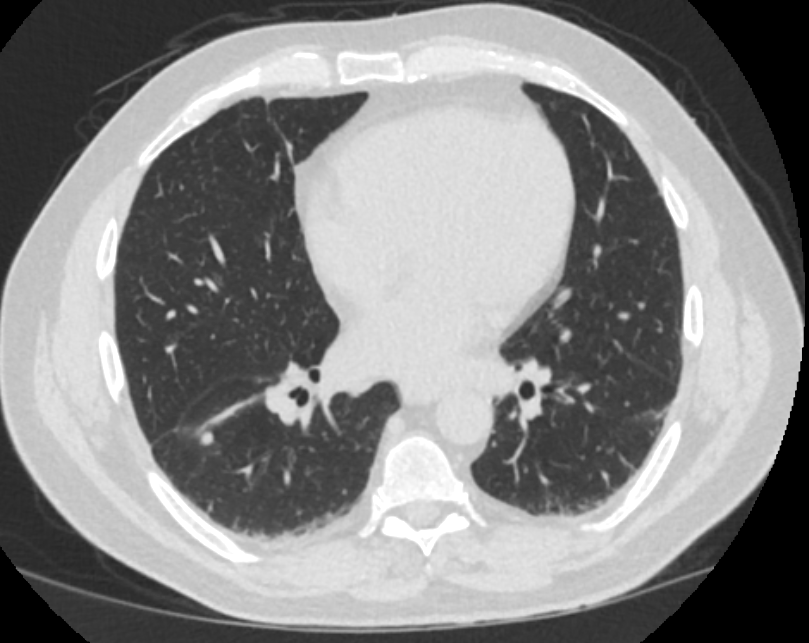
There is an incidental finding which requires further workup
There is a lung nodule in the right lower lobe.
View the full study if you'd like to take a look yourself.
Second Imaging Study
What is the next imaging study you will order?
No further imaging is required.
Well done. You were correct
What is your Diagnosis now that you have seen the imaging results?
The patient’s history of hyperparathyroidism (which leads to hypercalciuria) and celiac disease (which leads to hyperoxaluria) and the bright stone on CT suggest this is a calcium oxalate stone.
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
Considering the hydronephrosis secondary to the obstructing stone, the patient requires prompt treatment initialization.
Assessment and Plan
Please provide your assessment and plan for this patient
This is a young female presenting with renal colic, nausea, vomiting, and hematuria secondary to an obstructing UPJ stone leading to hydronephrosis. She requires urgent urological evaluation and will likely require a urologic procedure considering the size and sequelae secondary to the stone. She will also require imaging follow-up to assess the incidentally noted pulmonary nodules.
Lessons Learned:
- Non-contrast CT of the pelvis and abdomen is the gold standard for diagnosis of nephrolithiasis.
- Stones are most often lodged in the renal collecting system’s three sites of anatomical narrowing: ureteropelvic junction (UPJ), crossing of the ureter over the iliac vessels, and the ureterovesical junction (UVJ)
- Stones ≥ 10cm are unlikely to pass.
Socioeconomic Factors: Patients with lower educational levels and from regions with low mean income are more likely to have greater stone burden.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Contributors:
Kevin Pierre, MD - Editor
Robbie Slater, MD - Supervising Editor
Bayar Batmunh, MS - Coordinator
Next


{kind=link}
{kind=link}