Retake
A27) Epigastric pain with history of chronic pancreatitis
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a patient with epigastric pain.
- Review the DDx considerations in a patient with epigastric pain.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating a patient with epigastric pain.
History
A 52-year-old female presents to the emergency department with epigastric pain that started two hours ago. The pain is severe, sharp, and radiates to her back. She also endorses nausea and vomiting. She endorses a long history of frothy, pale, oily, foul-smelling stools. Chart review reveals a history of chronic pancreatitis and alcohol use disorder.
Physical Exam
BP: 128/83, HR 65, RR 16, Temp 98.9, O2 saturation 99%. Abdomen: Epigastric tenderness.
Labs
MCV 105 fl (nl 80-100 fl);
WBC within normal limits.
LFTs:
AST 110 U/L (nl: 8-33 U/L),
ALT 60 U/L (nl: 7-55 U/L).
Amylase: 135 U/L (nl: 40-140 U/L);
Lipase: 150 U/L (nl: 0-160 U/L);
LDH: 300 IU/L (nl: 105-333 IU/L).
Fasting blood glucose: 140mg/dL (nl: <100mg/dL)
Provisional Diagnosis
Select the Dx you believe is most appropriate
The patient’s presentation of severe sharp epigastric pain radiating to the back with steatorrhea in the setting of chronic pancreatitis likely reflects acute on chronic pancreatitis. The elevated LFTs with an AST/ALT ratio >2 and elevated MCV reflects the patient’s alcohol use disorder. The elevated fasting blood glucose is likely secondary to diabetes from pancreatic insufficiency secondary to the chronic pancreatitis. Lipase and amylase levels may be within normal limits in acute on chronic pancreatitis due to chronic pancreatic atrophy. Peptic ulcer disease and cholecystitis, however, are also on the differential diagnosis.
Well done. You were correct
Potential Acuity
What is your assessment of the likely acuity for this patient?
Well done. You were correct
The patient requires urgent workup and management.
First Imaging Study
What is the first imaging study you will order?
Considering that the lipase and amylase are within normal limits, the patient should undergo further workup to rule out pathologies other than pancreatitis. Contrast helps evaluate associated inflammation.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
CT Case
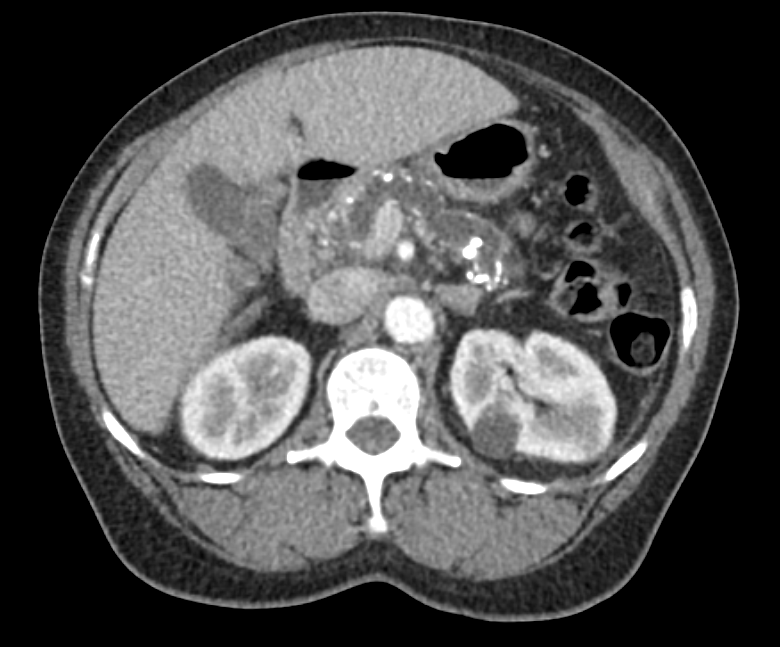
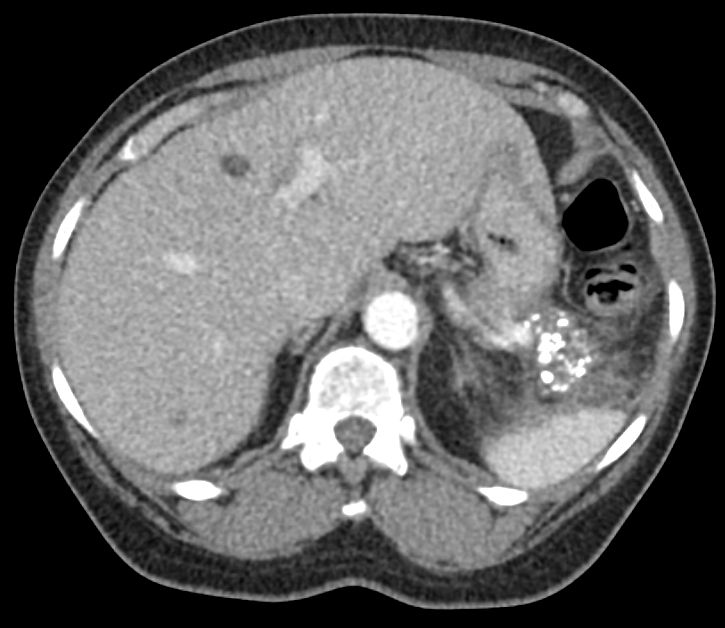
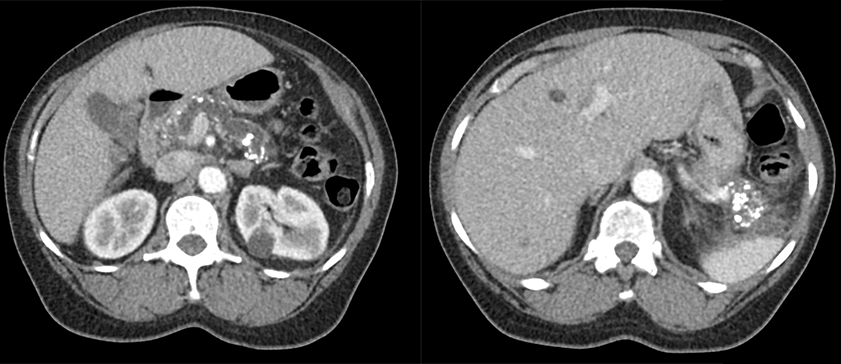
The pancreas is normal
There are extensive pancreatic calcifications and ductal dilatation reflecting the patient’s chronic pancreatitis.
View the full study if you'd like to take a look yourself.
Second Imaging Study
What is the next imaging study you will order?
The diagnosis is confirmed with the CT scan.
Well done. You were correct
What is your Diagnosis now that you have seen the imaging results?
The imaging findings of pancreatic atrophy, biliary ductal dilation, and pancreatic calcifications suggests chronic pancreatitis. The patient’s presentation and imaging revealing peripancreatic inflammation suggests an acute on chronic component.
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
The patient requires urgent management.
Assessment and Plan
Please provide your assessment and plan for this patient
The patient is 52-year-old female presenting with acute on chronic pancreatitis. The patient should be made NPO until their symptoms improve and should be admitted for aggressive fluid resuscitation and pain control. A low-fat diet will be trialed when their nausea and pain improve. She should also follow-up with an endocrinologist on an outpatient basis for further evaluation and management of diabetes.
Lessons Learned:
- Chronic alcoholism is a risk factor for pancreatitis.
- Chronic pancreatitis may appear on CT with pancreatitis calcifications and pancreatic ductal dilatation. Acute pancreatitis in comparison presents with pancreatic edema (parenchymal enlargement and density changes) and inflammation (peripancreatic fat stranding and indistinct margins).
- It is important to rule out pancreatitis with liquefactive necrosis (aseptic or infected/emphysematous), abscess formation, or hemorrhage.
Socioeconomic Factors:
- Mortality in patients with long-term cigarette use is most often secondary to cardiovascular disease and smoking rather than pancreatitis. Still, patients with chronic pancreatitis should be counseled on smoking and alcohol cessation to slow the development of the disease and development of other comorbidities.
- Alcoholic chronic pancreatitis is more common in the developed world when compared to undeveloped countries.
- In the United States, one in four patients diagnosed with chronic pancreatitis are readmitted within 30 days.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Next


{kind=link}
{kind=link}
{kind=link}
{kind=link}