Retake
A2) Abdominal pain and alternating bowel habits
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a patient with an incidental finding.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating a patient with an incidental finding.
History
A 27-year-old female with a history of anxiety, major depressive disorder, and fibromyalgia presents to clinic complaining of 8 months of abdominal pain. It is cramping, variable in intensity, and resolves with defecation. The pain has worsened over the past few months. She endorses darkened and thin stools with mucus over the past three weeks. She also often has alternating diarrhea and constipation. She has a family history of colorectal cancer (38 years old in brother and 39 years old in mother). She has regularly used OCPs for the past 5 years for uterine fibroids. She recently began taking iron tablets four weeks ago for anemia secondary to menorrhagia from her uterine fibroids. The symptoms are not worsened with gluten-containing foods.
Physical Exam
BP: 127/89, HR 78, RR 19, Temp 36.8, O2 saturation 100%.
Abdominal exam: mildly tender to palpation in right upper quadrant. Abdomen otherwise soft and nondistended.
Rectal exam: no blood in stool.
Labs
Fecal calprotectin: 70 mcg/g
Urine pregnancy test: negative
Fecal occult blood test negative.
Stool testing for giardia negative.
Celiac disease serologic testing negative.
CEA and CA 19-9 within normal limits.
Provisional Diagnosis
Select the Dx you believe is most appropriate
The patient’s variable cramping abdominal pain, alternating bowel habits, thin stools with mucous, increased fecal calprotectin, and associated comorbid conditions (anxiety, MDD, fibromyalgia) are consistent with a diagnosis of irritable bowel syndrome. The darkened stools may be secondary to iron tablets. The patient’s progressive abdominal pain and darkened stools are alarm features concerning for underlying organic disease. Colorectal cancer is possible considering the family history, but less likely considering her young age and negative serological markers.
Well done. You were correct
Potential Acuity
What is your assessment of the likely acuity for this patient?
Well done. You were correct
The patient’s current condition is not immediately life-threatening.
First Imaging Study
What is the first imaging study you will order?
An abdominal CT scan is a good initial test to rule out pathology like an obstructive colonic mass lesion.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
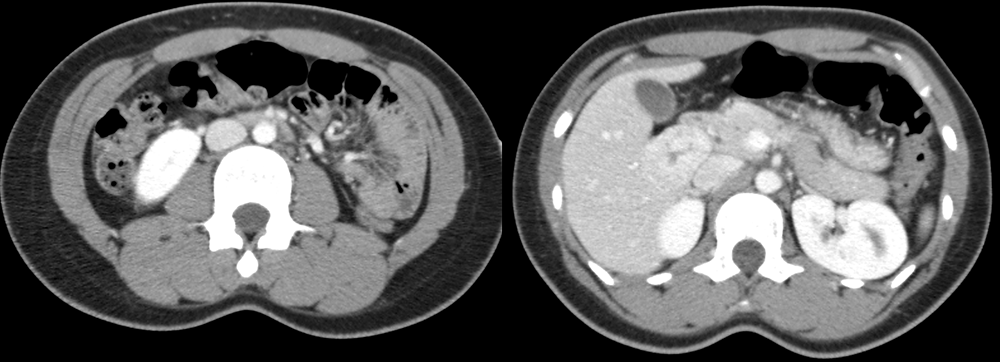
CT abdomen and pelvis
There is an incidentally noted liver lesion
There is an incidentally noted lesion in hepatic segment 5.
The liver lesion has a central scar
The liver lesion has a central, hypointense scar.
The liver lesion is enhancing
There is no obstructive or stricturing mass lesion. However, there is an incidentally noted enhancing liver lesion with a central scar.
View the full study if you'd like to take a look yourself.
Second Imaging Study
What is the next imaging study you will order?
An abdominal MRI can be obtained to further characterize the liver lesion.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
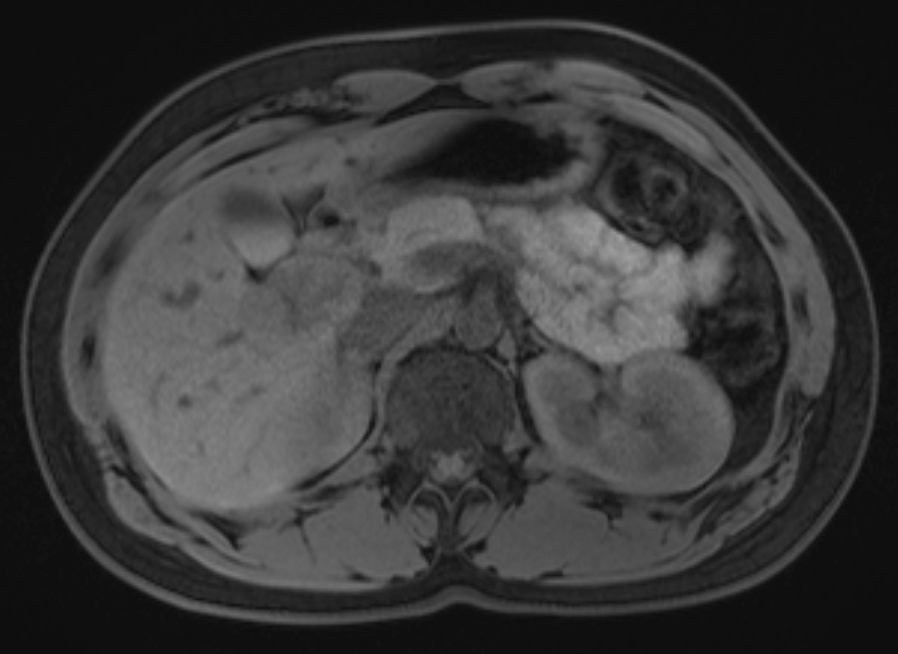
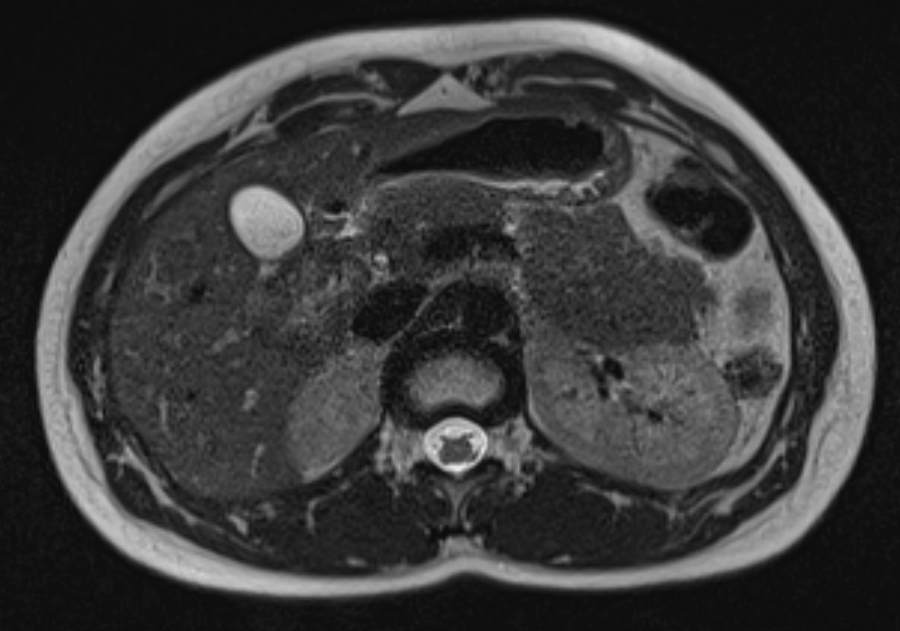
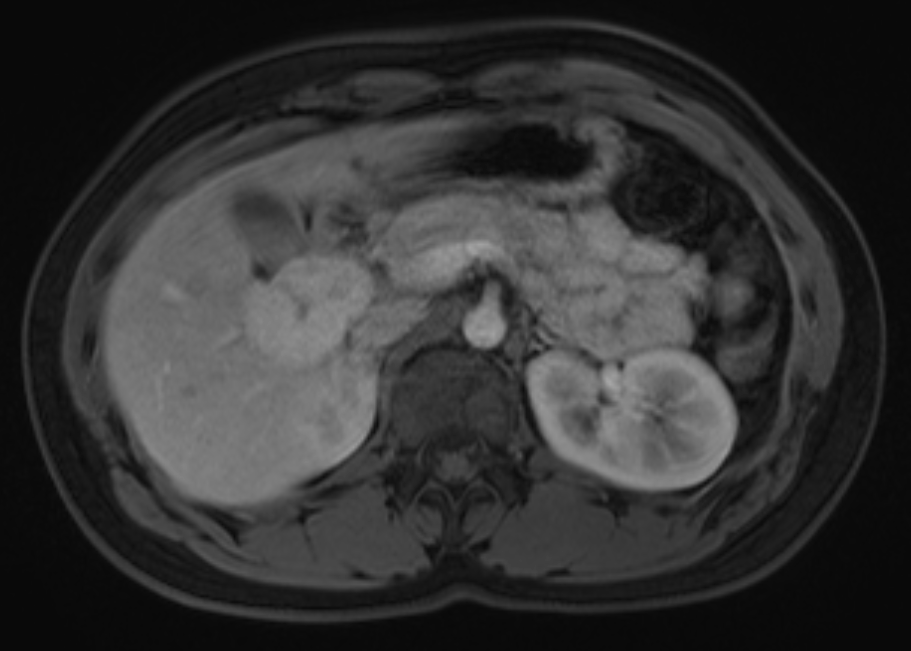
Abdominal MRI
The liver mass is iso/hypointense to the liver parenchyma on T1 imaging
The liver mass is both iso- and hypointense to the liver parenchyma on the T1-weighted image.
The liver mass is iso/hyperintense to the liver parenchyma on T2 imaging
The liver mass is both iso- and hyperintense to the liver parenchyma on the T1-weighted image.
View the full study if you'd like to like a look yourself
Third Imaging Study
What is the next imaging study you will order?
A diagnosis of FNH can be made as MRI is highly sensitive and specific for FNH.
What is your Diagnosis now that you have seen the imaging results?
The patient’s presentation is most consistent with irritable bowel syndrome. Because they presented with some red flag symptoms, imaging was obtained and incidentally revealed a focal nodular hyperplasia.
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
The patient’s condition is not immediately life-threatening. Compared to hepatic adenomas, FNH has a significantly lower risk of bleeding.
Assessment and Plan
Please provide your assessment and plan for this patient
The patient is a 27-year-old female presenting with variable, cramping abdominal pain, and abnormal bowel movements. She should be referred to gastroenterology for this suspected irritable bowel syndrome and for consideration of early colorectal cancer screening considering her significant family history. An incidental focal nodular hyperplasia was noted on imaging. She will require regular imaging follow-up and consideration for intervention if this becomes symptomatic.
Lessons Learned:
- Focal nodular hyperplasia is a regenerative, non-cancerous lesion that most often develops in young females.
- Unlike hepatic adenomas, OCP use is not associated with the development of FNH. However, their use is associated with increased size of the FNH lesion.
- FNH appears on CT and MRI as an enhancing lesion with a central scar. It is iso- to hypointense on T1 weighted images and iso- to hyperintense on T2 weighted images.
Socioeconomic Factors: Patients presenting with symptoms and signs consistent with irritable bowel syndrome do not require imaging unless they also have red flag symptoms (age 50+, bloody/dark stools, progressive abdominal pain, weight loss, nocturnal diarrhea).
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Contributors:
Kevin Pierre, MD - Editor
Robbie Slater, MD - Supervising Editor
Bayar Batmunh, MS - Coordinator
Next


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}