Pediatric Pelvic Trauma and Pain (Radiograph)
Pediatric Pelvic Trauma and Pain (Radiograph)
Search Pattern Assist ?History
Exam
2. Frontal view of the pelvis and views of the left/right hip.
3. Frontal and bilateral Judet views of the pelvis.
4. Frontal, inlet, and outlet views of the pelvis.
5. Frontal and bilateral frog-leg lateral views of the pelvis.
Prior Study
Findings
IMAGE QUALITY
Portions of the patient’s anatomy are excluded from the field of view. [Yes/No]
There are external structures overlying the patient’s pelvis, such as a backboard. [Yes/No]
The image is rotated. [Yes/No]
VISUALIZED LUMBAR SPINE
There are compression fractures. [Yes/No]
There are transverse process fractures. [Yes/No]
There is lumbar spine degeneration. [Yes/No]
SACRUM and SACROILIAC JOINTS
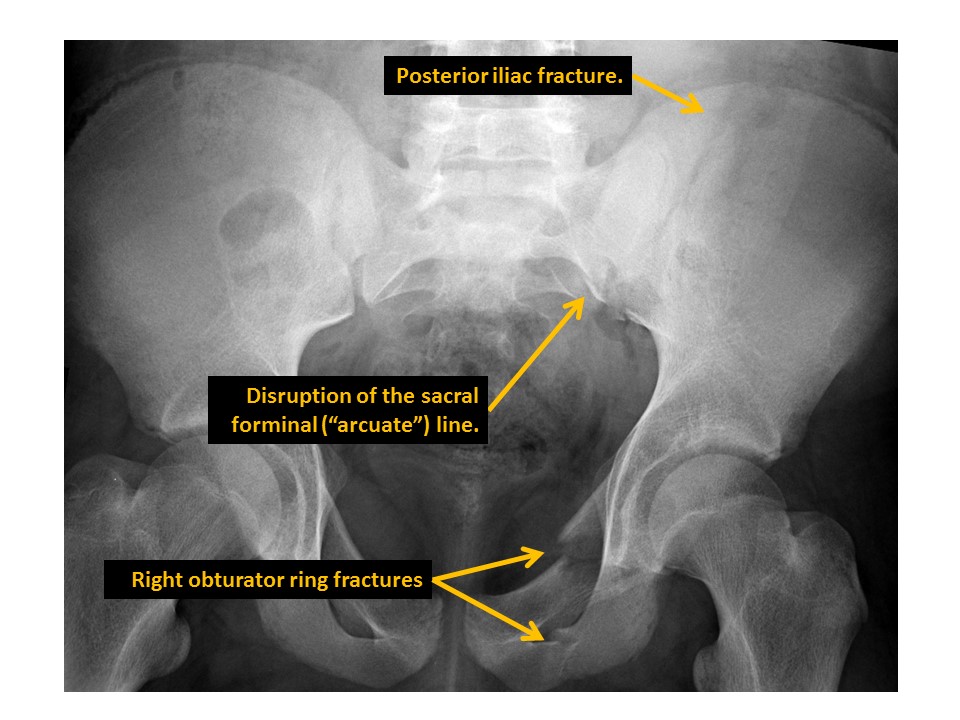
There are displaced fractures or disrupted/asymmetric foraminal arcs. [Yes/No]
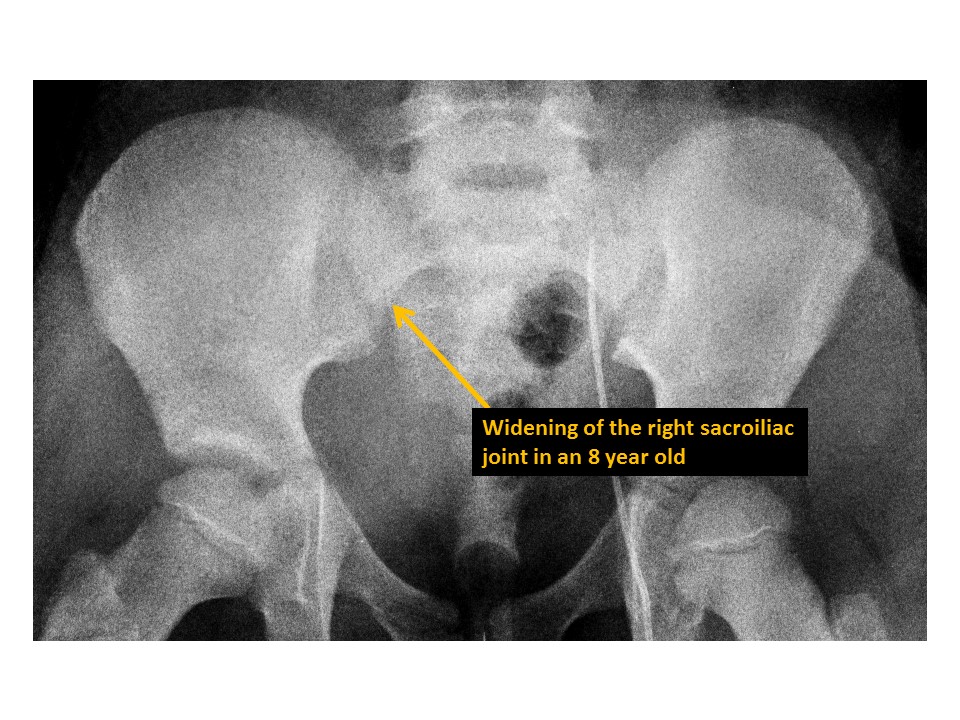
The sacroiliac joints are widened and asymmetric. [Yes/No]
There is malalignment at the inferior margin of the sacroiliac joints. [Yes/No]
There are radiographic findings of sacroiliac inflammation or degeneration. [Yes/No]
PUBIC SYMPHYSIS and RAMI
The pubic symphysis is widened or vertically incongruent. [Yes/No]
There are radiographic findings of pubic symphysis inflammation or degeneration. [Yes/No]
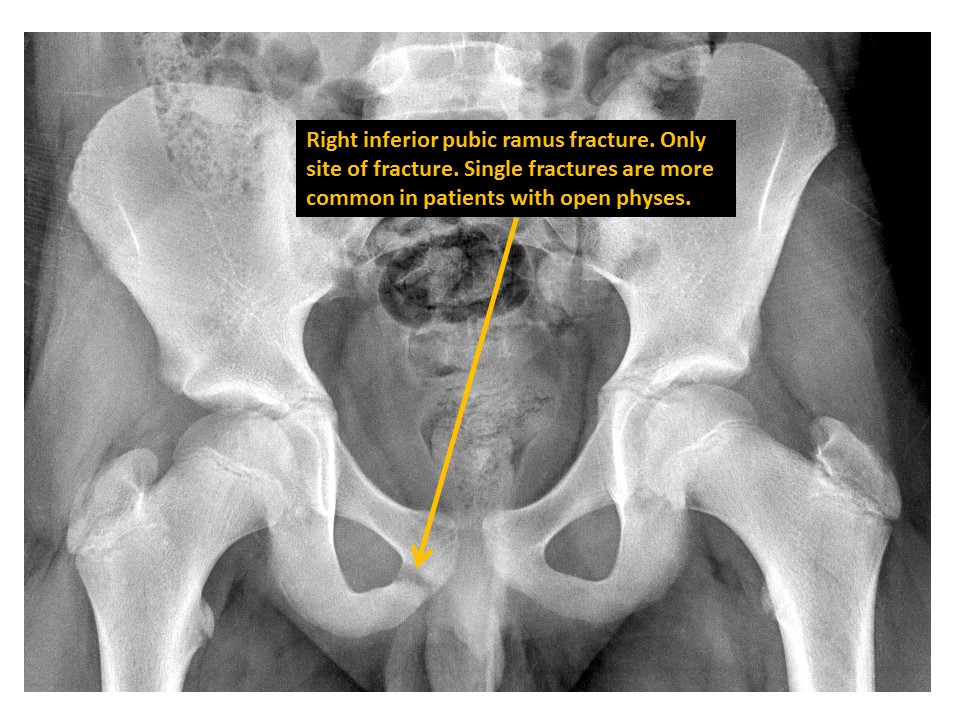
There is a pubic ramus fracture. [Yes/No]
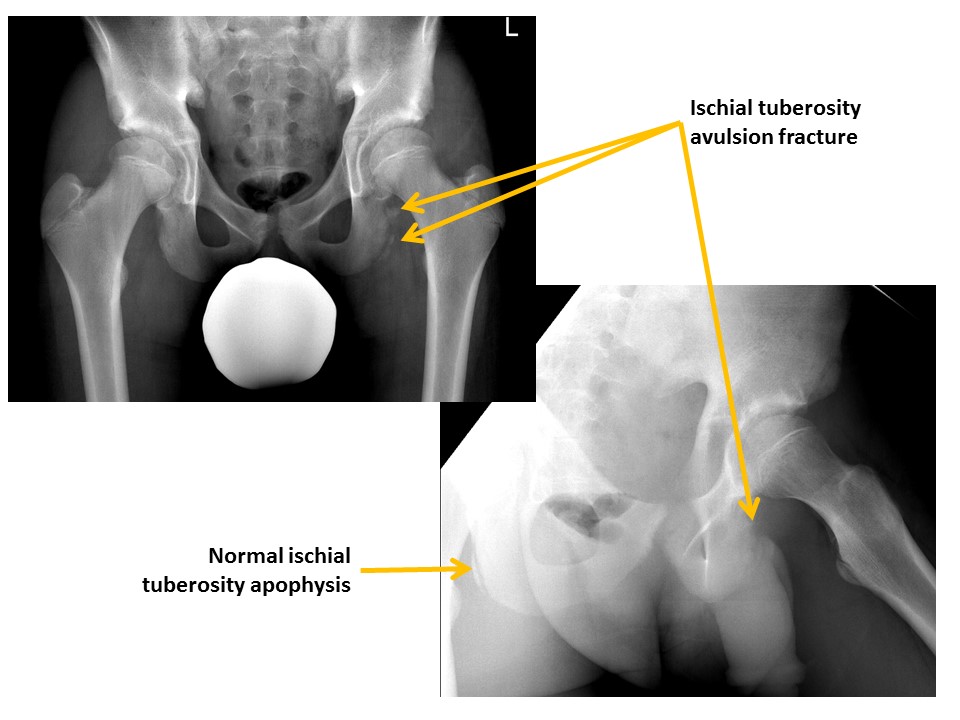
There are avulsion fractures at the ischial tuberosities. [Yes/No]
ILIAC BONES
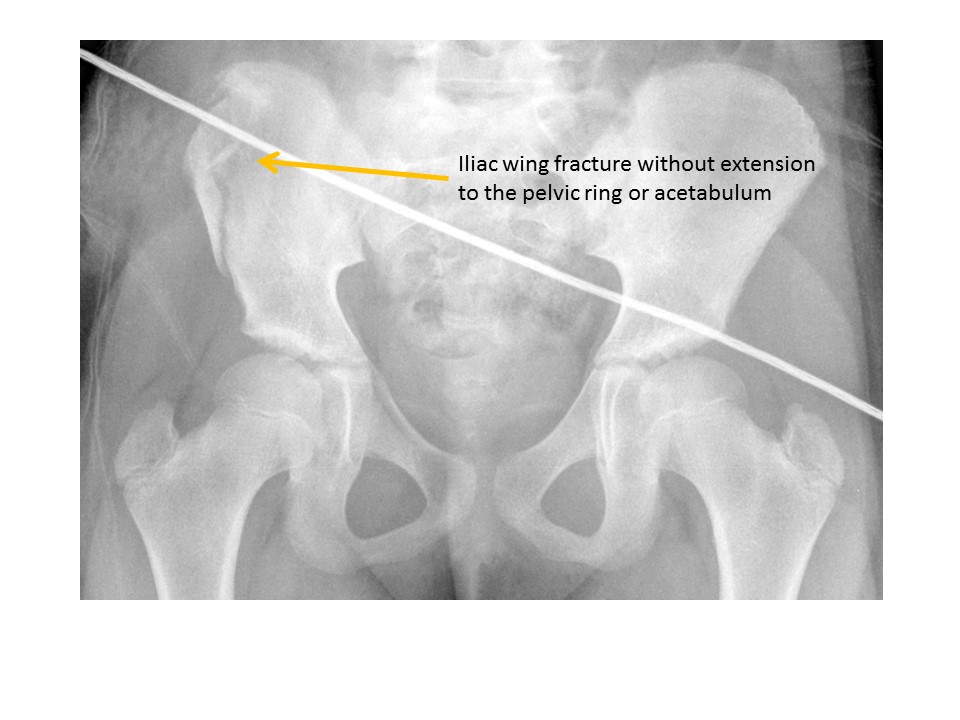
Iliac wing fractures are present. [Yes/No]
Posterior iliac bone fractures are present. [Yes/No]
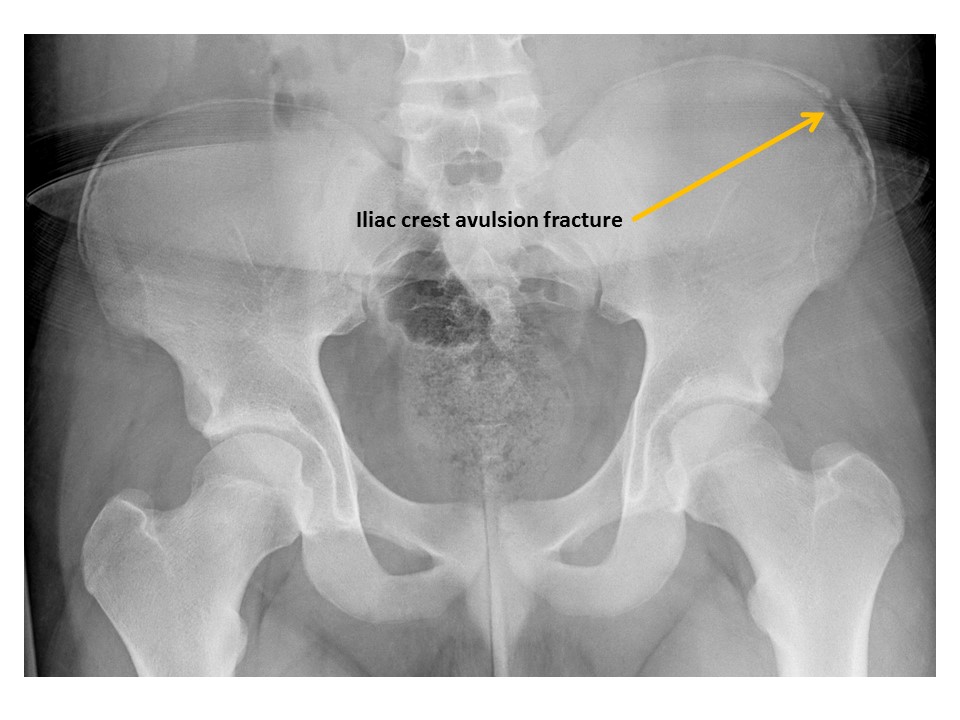
Iliac crest avulsion fractures are present. [Yes/No]
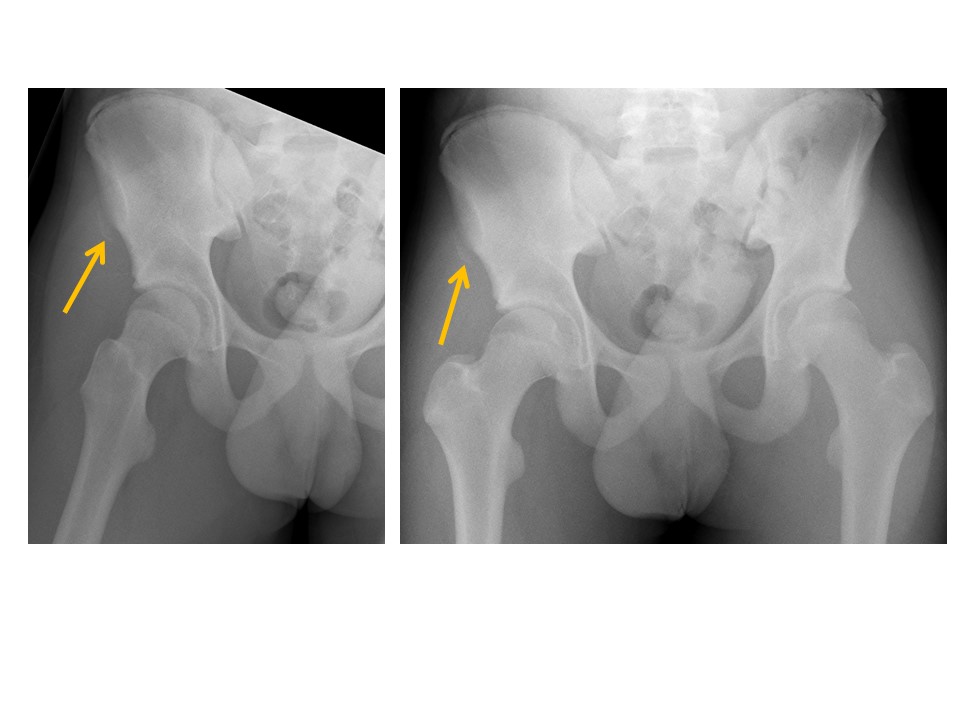
Anterior superior iliac spine avulsion fractures are present. [Yes/No]
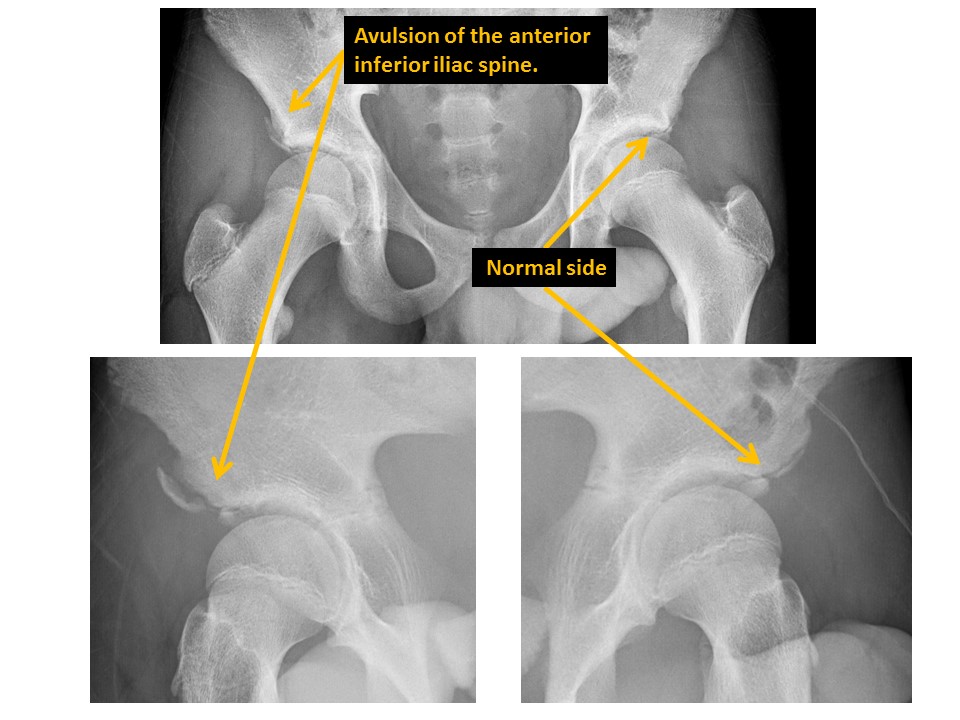
Anterior inferior iliac spine avulsion fractures are present. [Yes/No]
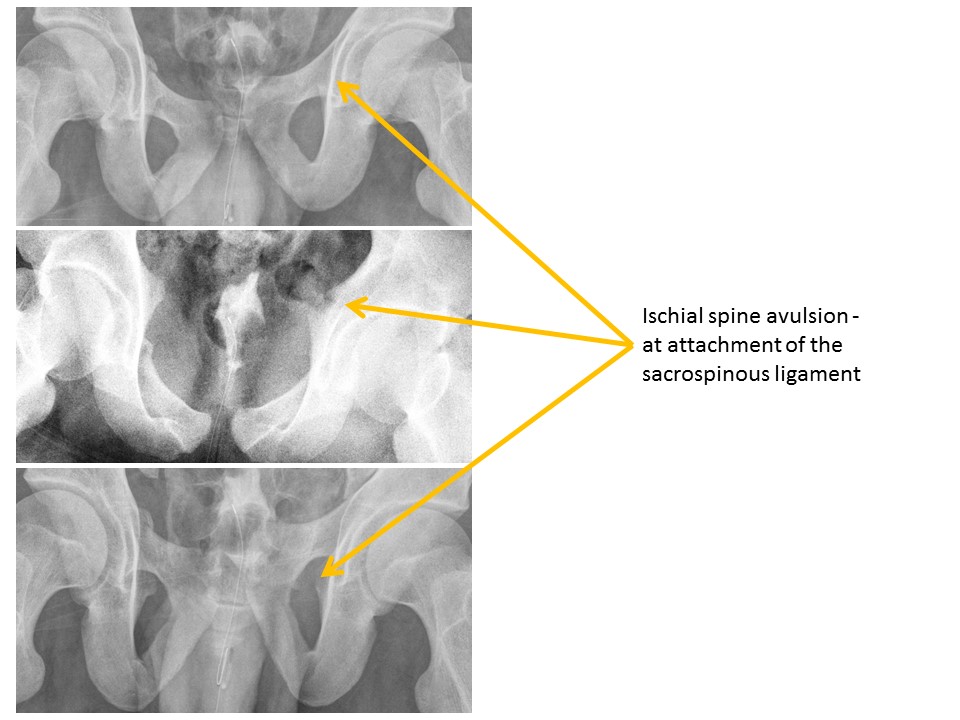
Ischial spine avulsion fractures are present. [Yes/No]
HIPS/PROXIMAL FEMURS
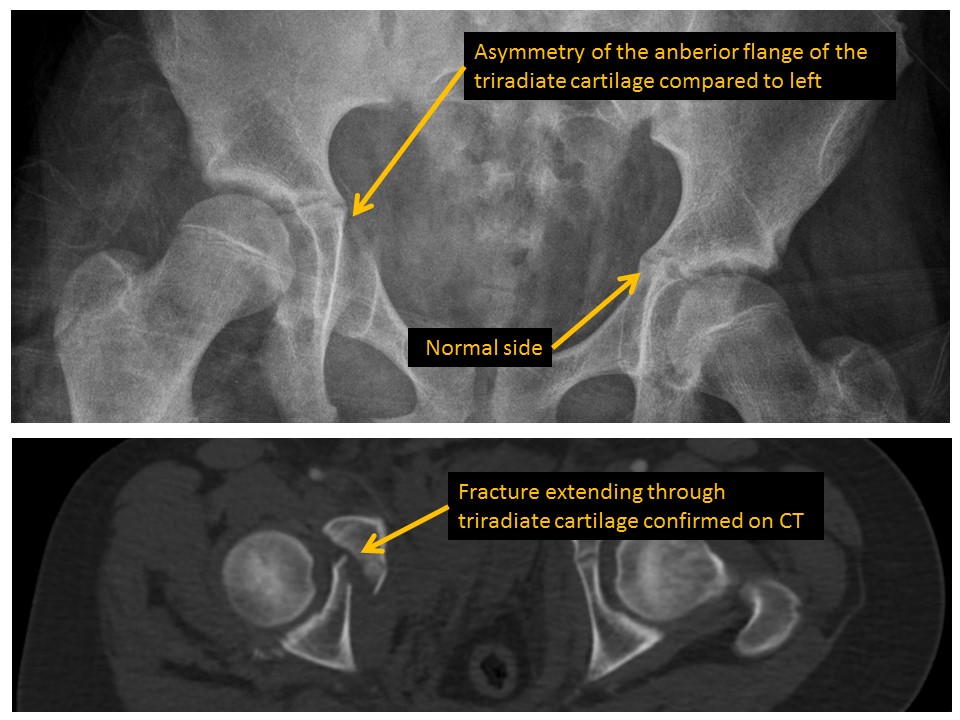
Triradiate cartilages (if open) are asymmetric or disrupted. [Yes/No]
Ilioischial lines are disrupted. [Yes/No]
Iliopubic (iliopectineal) lines are disrupted. [Yes/No]
Anterior walls of the acetabula (if ossified) are disrupted. [Yes/No]
Posterior walls of the acetabula (if ossified) are disrupted. [Yes/No]
Anterior walls of the acetabula (if ossified) are lateral to the posterior walls (“crossover sign”). [Yes/No]
Acetabular roofs are discontinuous. [Yes/No]
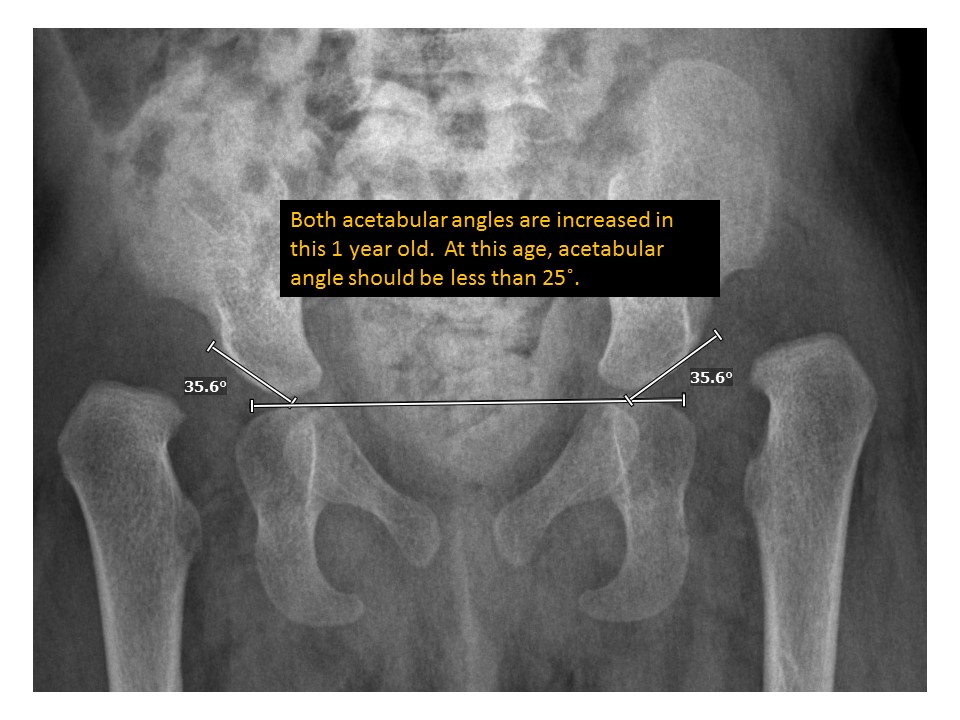
Acetabular angles are abnormal. [Yes/No]
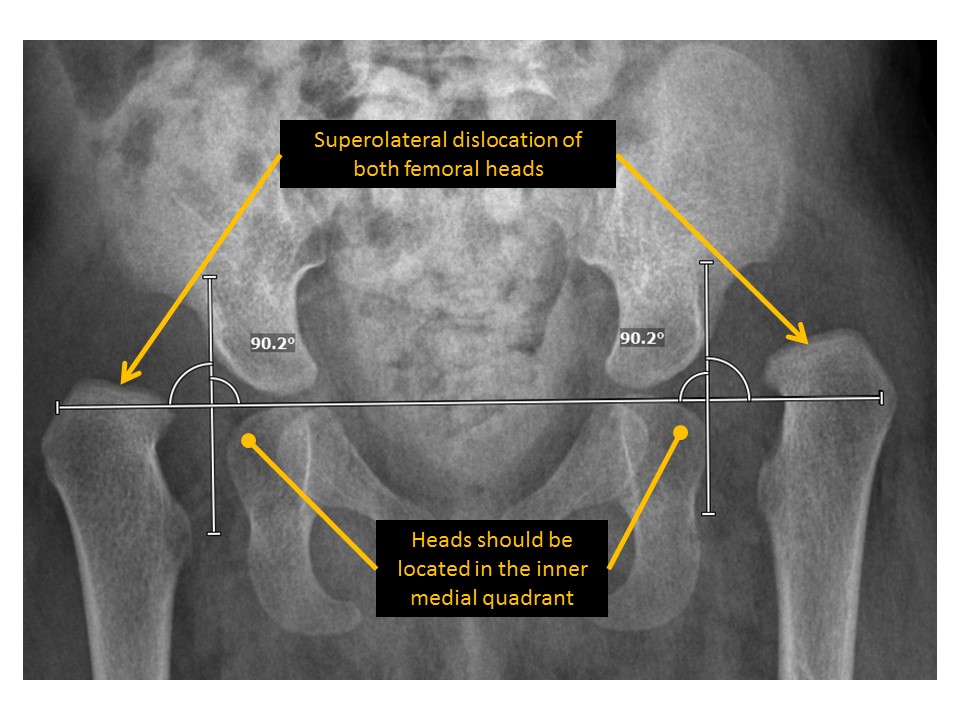
There is hip dislocation or subluxation. [Yes/No]
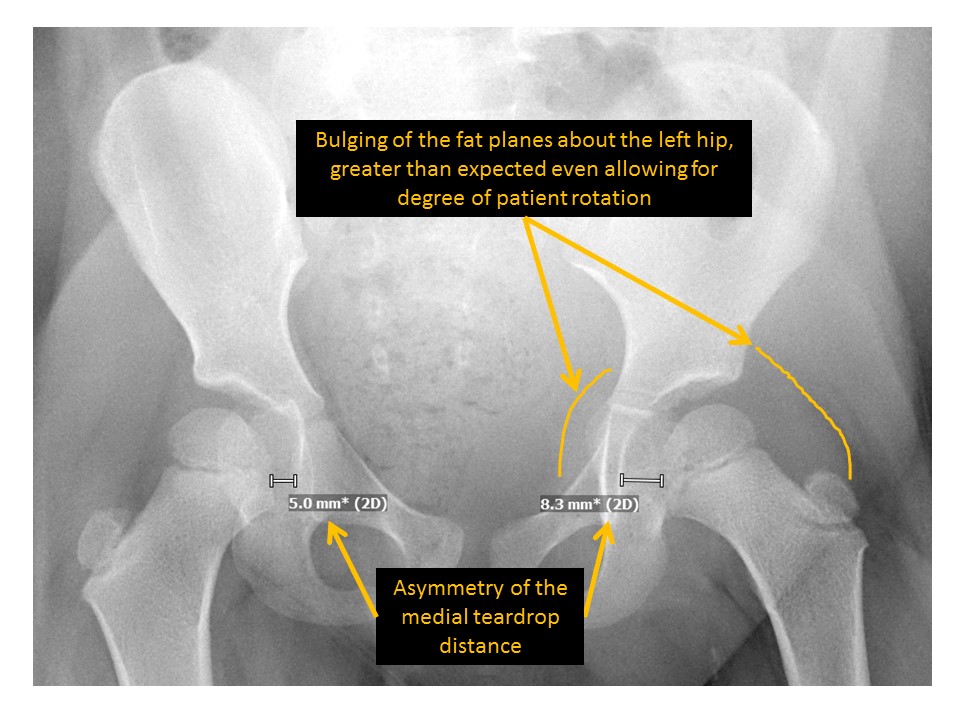
The teardrop distance is asymmetric. [Yes/No]
There is bulging of the fat planes about the hips. [Yes/No]
There are radiographic findings of hip osteoarthritis or inflammation. [Yes/No]
The cortices of the femoral heads are irregular or indistinct. [Yes/No]
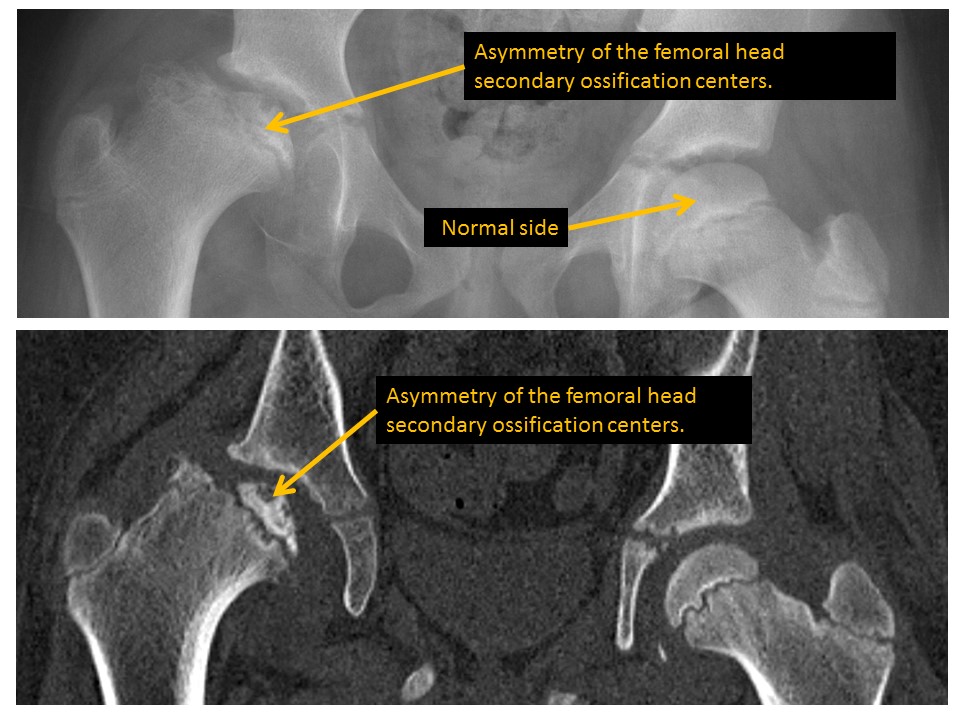
There is abnormal osseous density of the femoral epiphyseal ossification centers. [Yes/No]
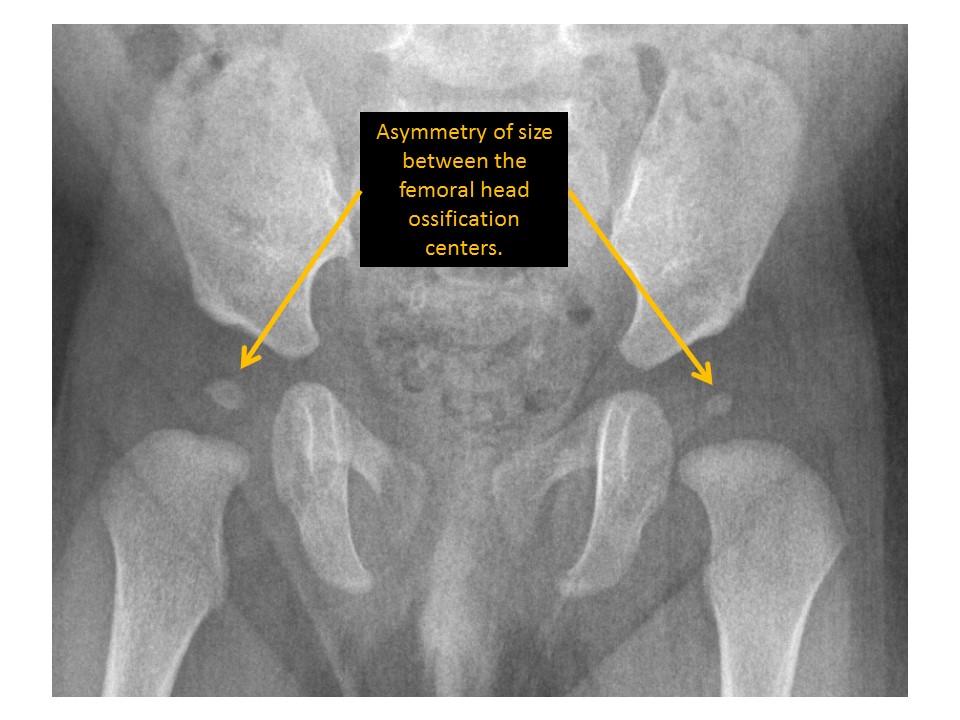
Femoral epiphyseal ossification centers are asymmetric in size. [Yes/No]
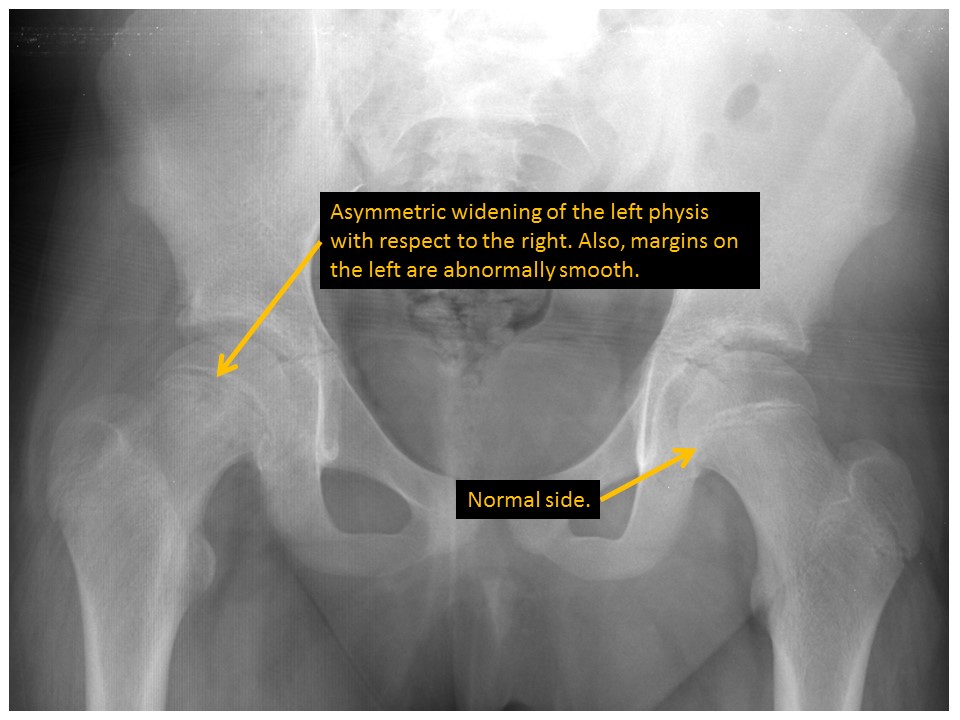
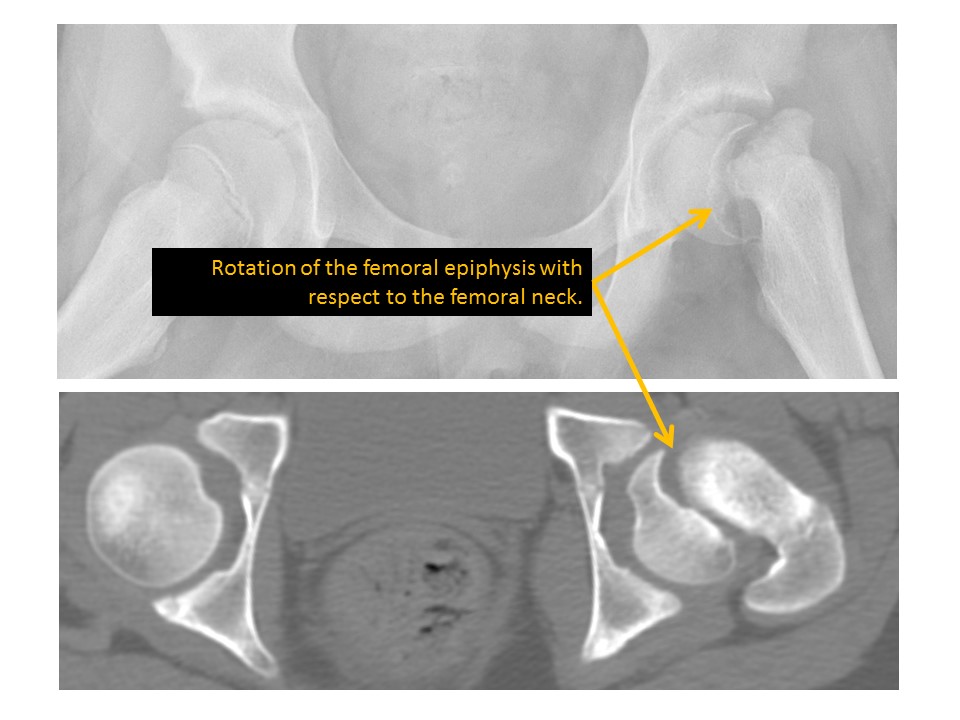
The proximal femoral physes are widened or abnormally smooth or irregular in contour. [Yes/No]
Klein lines asymmetrically cross the femoral epiphyses or there is displacement of the femoral epiphyses with respect to the femoral necks. [Yes/No]
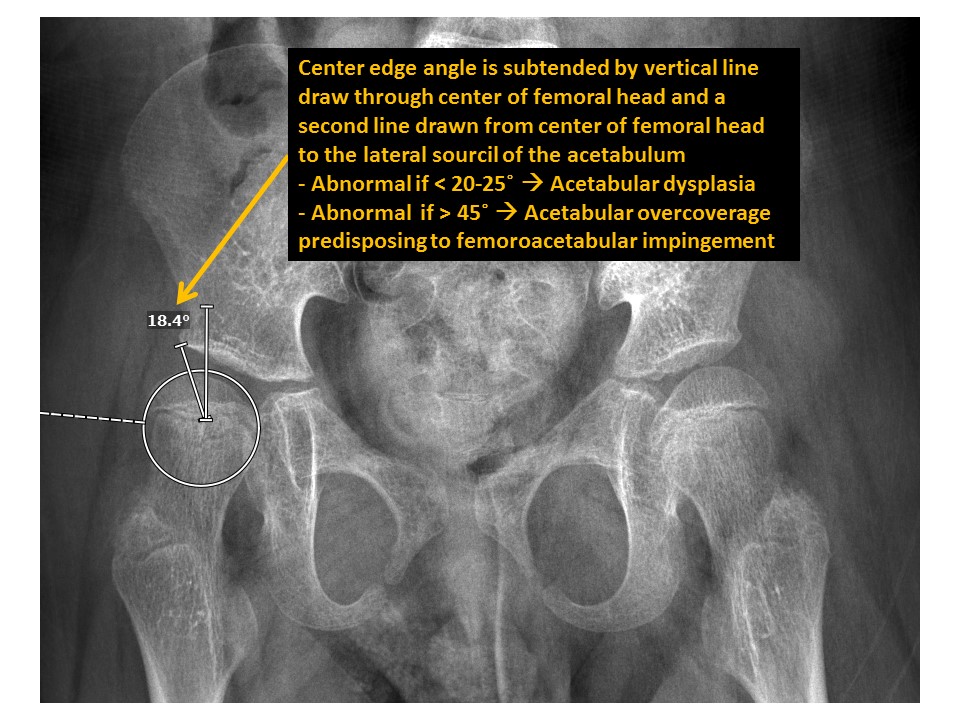
The center edge angle of the femoral heads is abnormal. [Yes/No]
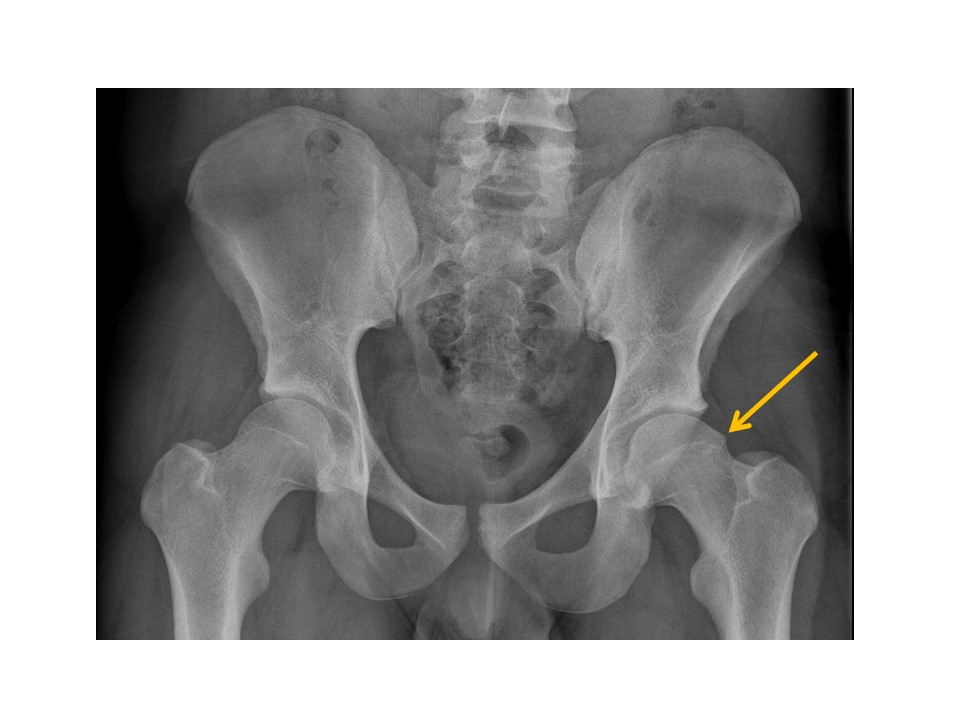
There is osseous prominence at the lateral femoral head/neck junctions. [Yes/No]
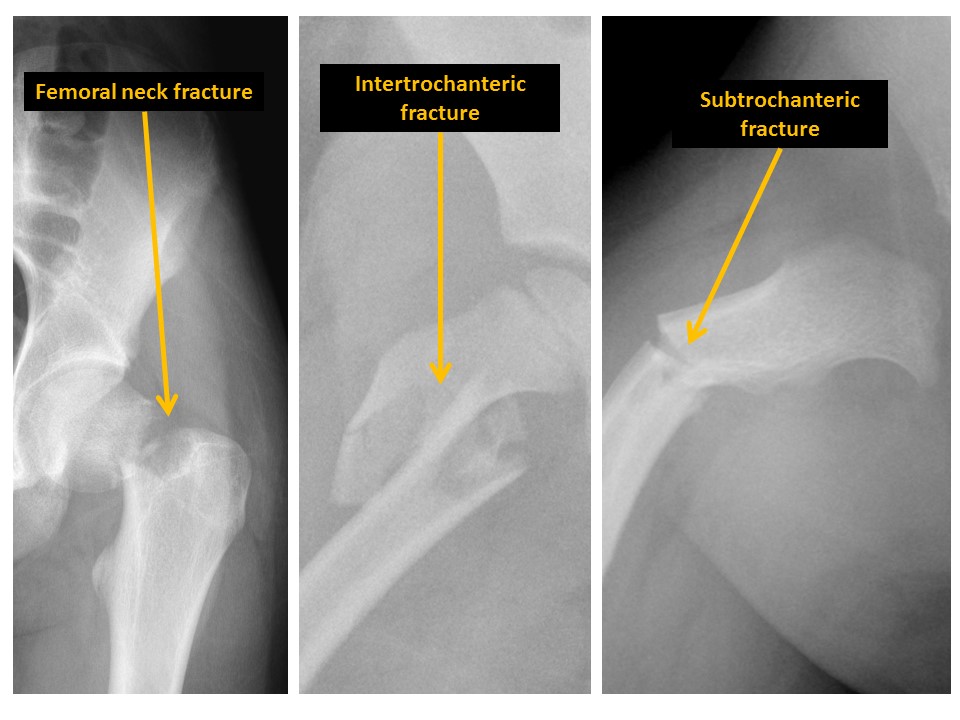
There are fractures of the femoral neck, intertrochanteric region, or subtrochanteric region. [Yes/No]
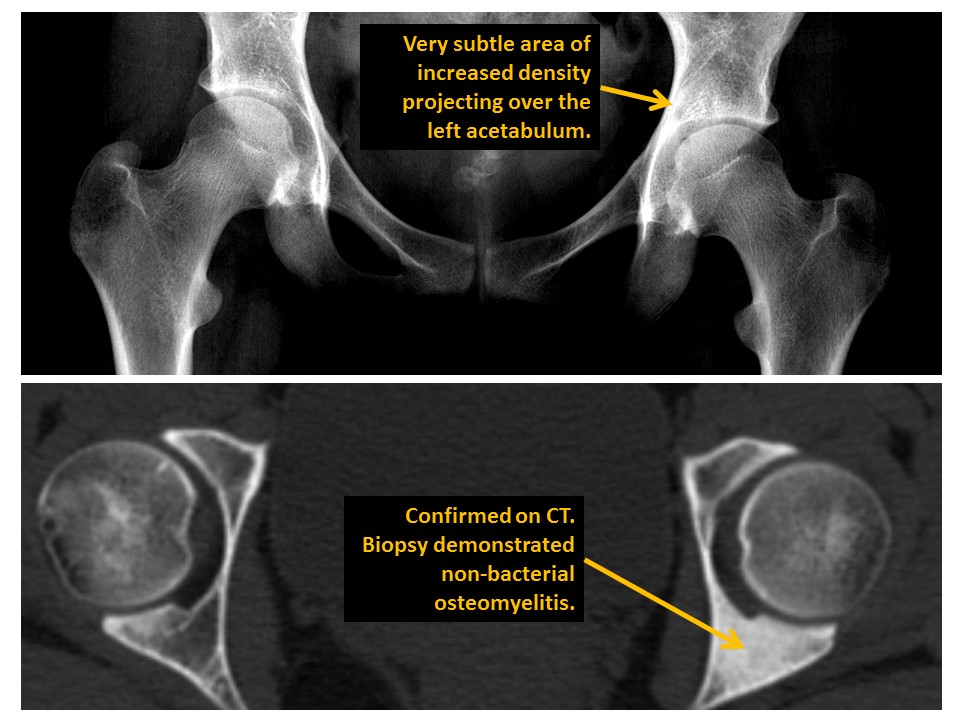
The trabecular pattern of the proximal femurs is abnormal. [Yes/No]
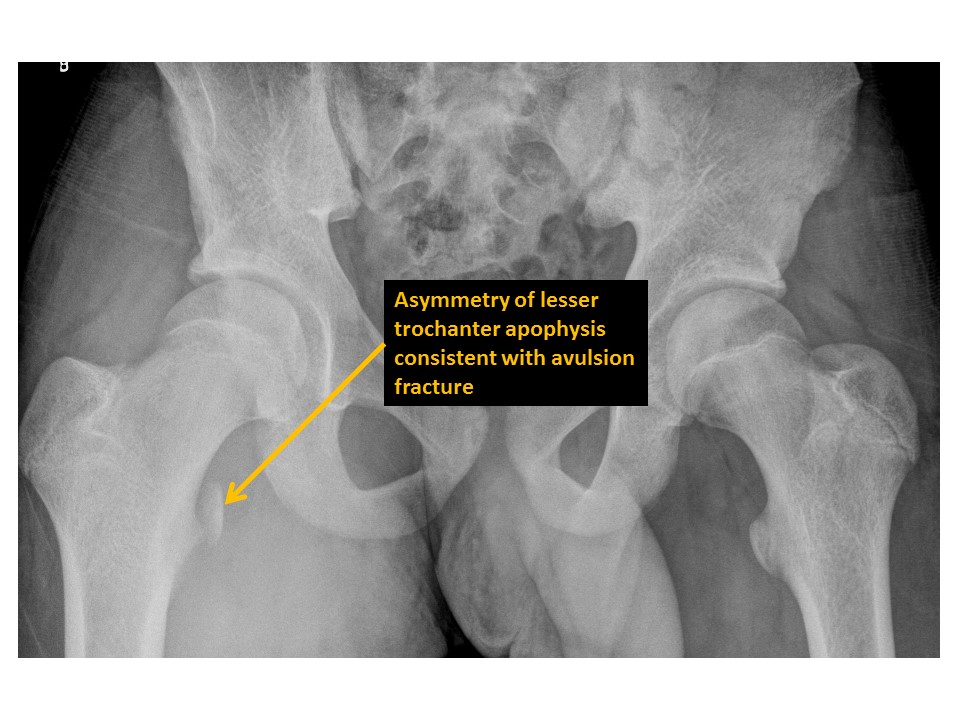
There are avulsion fractures of the greater or lesser trochanters. [Yes/No]
MISCELLANEOUS
The osseous mineralization is diffusely abnormal. [Yes/No]
SOFT TISSUES
There are radio-opaque foreign bodies, lacerations, or soft tissue swelling. [Yes/No]
There are other incidental soft tissue abnormalities. [Yes/No]
Impression
Pediatric Pelvis Xray
-
1-Hip/pelvis fracture/malalignment as discussed above.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}