Retake
N3) Progressive numbness, burning, and weakness of the upper extremities
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a patient with a radiculopathy.
- Review the DDx considerations in a patient with radiculopathy.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating patients with a radiculopathy.
History
A 23-year-old woman presents to her primary care physician with a five-month history of progressive numbness, burning, and weakness in her hands and arms. The patient denies any history of trauma, infection, incontinence, fatigue, visual disturbances, balance problems, and is otherwise healthy.
Physical Exam
BP: 128/72, HR 84, RR 16, Temp 98 F, O2 saturation 98%. Decreased sensation to light touch and temperature in both hands and forearms in a cape-like distribution. Motor strength is 4/5 in both upper extremities with decreased handgrip strength. Deep tendon reflexes are normal. Hoffman's sign is present bilaterally. No gait disturbances.
Labs
None
Provisional Diagnosis
Select the Dx you believe is most appropriate
Based on her age, the progressive course of her cervical myelopathy, and the nature and “cape-like” distribution of her sensory deficits, a cervical cord syrinx is the most probable diagnosis.
Well done. You were correct
Potential Acuity
What is your assessment of the likely acuity for this patient?
Well done. You were correct
The patient requires routine workup as their condition is not immediately life-threatening.
First Imaging Study
What is the first imaging study you will order?
Given the clinical presentation and physical exam findings, a Cervical Spine MRI would be the most appropriate initial imaging study to evaluate for potential spinal cord pathology, such as a syrinx.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
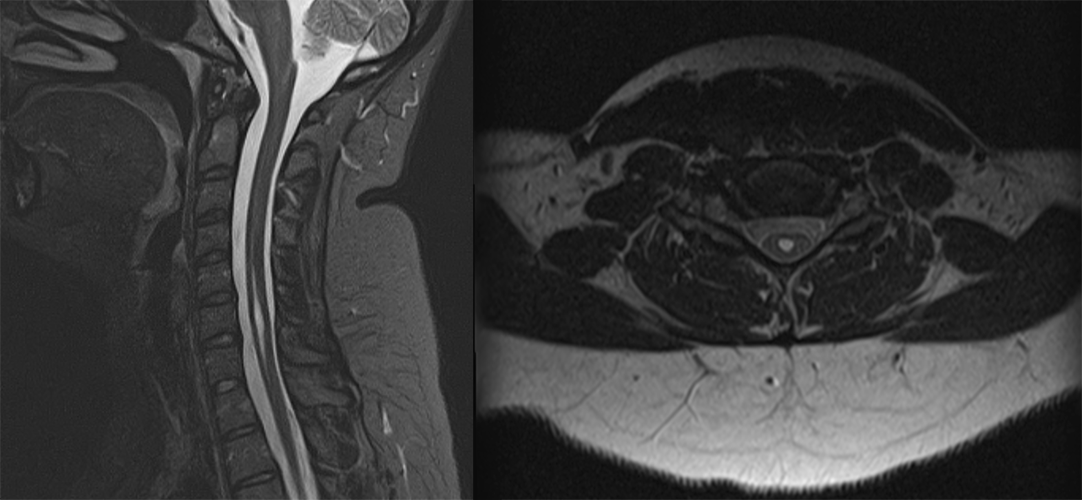
C-spine MRI
There is fluid within which part of the spinal cord?
The cervical portion of the spinal cord shows the presence of fluid in the central canal, specifically from C5-C7.
Is there evidence of external cervical cord compression?
The MRI does not show any signs of external cervical cord compression, such as from a herniated disc or cervical stenosis.
View the full study if you'd like to take a look yourself.
What is your Diagnosis now that you have seen the imaging results?
The fluid filled expansion of the central canal of the cervical spinal cord, confirms the diagnosis of a syringomyelia.
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
The patient requires routine workup as their condition is not immediately life-threatening.
Assessment and Plan
Please provide your assessment and plan for this patient
The patient is a 23-year-old male who presented with symptoms suggestive of cervical myelopathy. The MRI findings have confirmed the presence of a cervical cord syrinx from C5-C7. A neurosurgery consultation should be placed to determine the need for surgical intervention, like a shunt placement, versus conservative management. The patient should also be administered analgesics for pain management.
Lessons Learned:
- A syrinx is a fluid-filled cavity within the spinal cord (syringomyelia) or brain stem (syringobulbia).
- The clinical presentation of syringomyelia can vary depending on the location and extent of the syrinx. This patient with a cervical syrinx presented with cervical myelopathy in a “cape-like” distribution.
- Whether managed conservatively or surgically, regular follow-up is important to monitor the status of the syrinx.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Next


{kind=link}