Retake
N18) Hearing loss, tinnitus, and vertigo
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Recognize the importance of consulting with diagnostic radiologists in the evaluation of patients with vertigo and hearing loss.
- Develop an understanding of the differential diagnosis considerations in patients with vertigo and hearing loss.
- Demonstrate knowledge of appropriate imaging modalities and their respective imaging findings in the evaluation of patients with vertigo and hearing loss.
History
A 70-year-old female presents to the clinic with a complaint of progressive left-sided hearing loss and tinnitus over the last 11 months. The patient also reports occasional episodes of vertigo and balance issues.
Physical Exam
BP: 125/78, HR 95, RR 16, Temp 98F, O2 saturation 96% on room air. On neurological examination, the patient has grossly diminished left-sided hearing, with sound lateralizing to the right ear when a tuning fork is placed at the midline of the patient's head. Bone conduction is greater than air conduction on the left side, while air conduction is greater than bone conduction on the right side. The patient also exhibits left-sided upper and lower facial weakness, an unsteady and wide-based gait, and a tendency to veer to the left. Additionally, the patient veers to the left side when asked to stand with her feet together and eyes closed.
Labs
Laboratory studies, including a comprehensive metabolic panel and B12 levels, are within normal limits.
Provisional Diagnosis
Select the Dx you believe is most appropriate
This patient’s presentation is highly suggestive of a vestibular schwannoma considering the sensorineural hearing loss (Weber test lateralizing to the right and abnormal left sided Rinne test), and CNVII involvement (left panfacial weakness).
Well done. You were correct
Potential Acuity
What is your assessment of the likely acuity for this patient?
Well done. You were correct
This patient requires routine, but expedited workup, considering that their suspected condition is not immediately life-threatening.
First Imaging Study
What is the first imaging study you will order?
A brain MRI is the preferred initial imaging modality for evaluating patients with vertigo and hearing loss due to its superior tissue resolution and ability to directly visualize the cranial nerves and detect the presence of a vestibular schwannoma. Additionally, brain MRI does not use ionizing radiation, making it safer for patients, especially those who may require repeated imaging studies. In addition to detecting vestibular schwannomas, a brain MRI can also help rule out other potential etiologies, such as multiple sclerosis, and provide detailed information about the size and location of any identified lesion to guide further management decisions.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
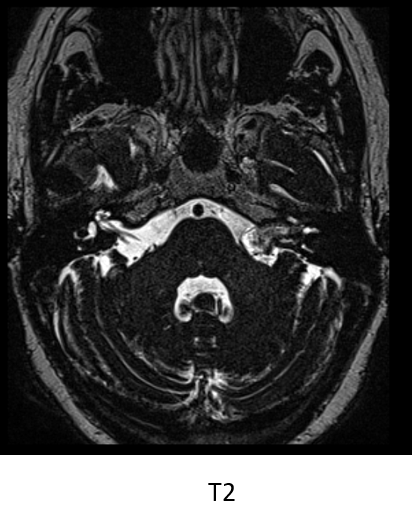
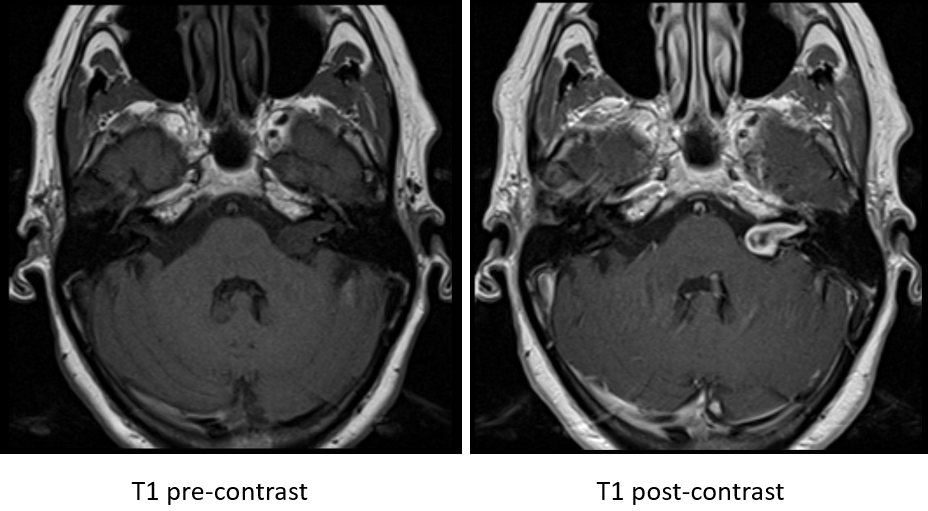
Brain MRI
In which internal acoustic canal is the mass located?
The mass is in the left internal acoustic canal extending into the cerebellopontine angle.
Does the mass have any enhancing features?
The mass heterogeneously enhances with contrast administration.
View the full study if you'd like to take a look yourself.
Second Imaging Study
What is the next imaging study you will order?
No further imaging is needed.
Well done. You were correct
What is your Diagnosis now that you have seen the imaging results?
The patient’s history, physical exam, and imaging findings are highly suggestive of vestibular schwannoma.
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
This patient requires routine, but expedited workup.
Assessment and Plan
Please provide your assessment and plan for this patient
The patient is a 70-year-old female presenting with progressive left-sided sensorineural hearing loss, tinnitus, vertigo, balance issues, and left sided facial weakness. Imaging confirmed the presence of a left-sided cerebellopontine angle tumor, consistent with a vestibular schwannoma. The patient should be referred to a neurotologist for further evaluation and management. There, they will discuss treatment options, including observation, radiation therapy, and surgical resection.
Lessons Learned:
- Vestibular schwannomas typically originate from Schwann cells in the vestibular portion of the vestibulocochlear nerve (cranial nerve VIII) within the internal auditory meatus.
- Facial weakness may occur in patients with vestibular schwannomas due to the mass effect on the facial nerve (cranial nerve VII), which runs in close proximity to the vestibulocochlear nerve in the internal auditory meatus and cerebellopontine angle.
- For patients with smaller vestibular schwannomas and minimal hearing loss, a conservative approach involving observation and regular follow-up may be appropriate to monitor for changes in tumor size and symptom progression.
Socioeconomic Factors: Vestibular schwannomas have an incidence of about 1 per 100,000 person-years in the U.S. Rates are higher in Taiwan and among Asian Pacific Islanders, while they are lower in Hispanics and African Americans.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Next


{kind=link}
{kind=link}