C1) Fever, Cough, and Leukocytosis
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a patient with fever and cough.
- Review the DDx considerations in fever and cough.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating patients with fever and cough.
History
Physical Exam
Labs
Provisional Diagnosis
Potential Acuity
What is your assessment of the likely acuity for this patient?
First Imaging Study
What is the first imaging study you will order?
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
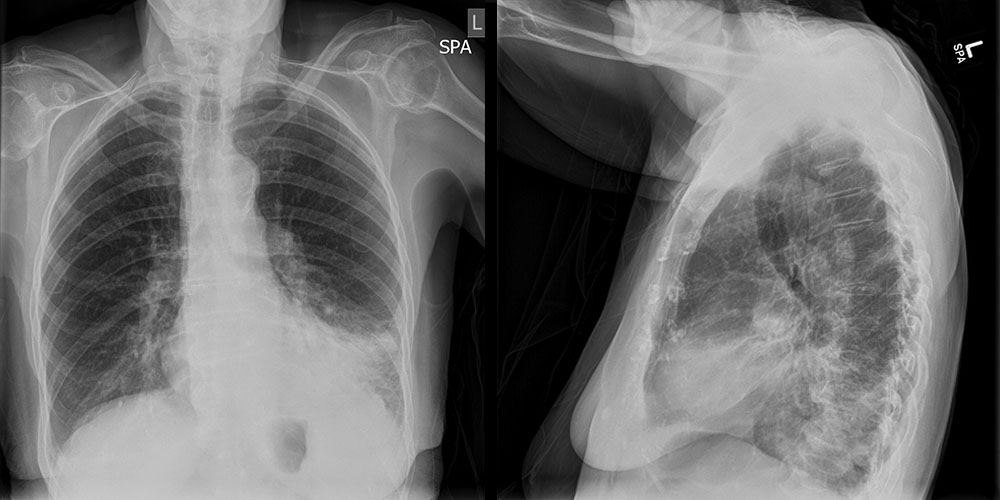
Chest PA and Lateral
What best describes the findings on the chest radiograph?

Watch our video
Second Imaging Study
What is the next imaging study you will order?
What is your Diagnosis now that you have seen the imaging results?
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
Assessment and Plan
Please provide your assessment and plan for this patient
Lessons Learned: Several imaging features support the diagnosis of lobar pneumonia. (1) Airspace opacities (fluffy infiltrates with indistinct margins), which represent alveoli filling with exudate. (2) Air bronchograms (dark, streaky lines within the opacified area), which represent bronchi made more visible by surrounding alveoli filled with exudate. (3) Silhouette sign, which occurs when the opacified lung becomes a similar density to the diaphragm, heart border, or mediastinum, making them invisible. (4) Spine sign; the spine normally becomes darker when viewed from the top to bottom on a lateral chest radiograph. When there is an overlying infiltrate, the spine will appear whiter.
Socioeconomic Factors: (1) In a patient with a similar presentation, some centers may elect to begin with a CT scan. However, a chest X-ray is more cost-effective and minimizes radiation exposure.(2) In this case, a follow up X-ray may be considered to follow for resolution if there is a concern that this is a post-obstructive pneumonia secondary to an endobronchial cancer. However, if the patient is unlikely to follow up, we should consider performing a CT scan prior to discharge.(3) If a younger patient without comorbidities presents similarly, we may treat more conservatively by sending them home with antibiotics and close clinical follow up.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Contributors:
Kevin Pierre, MD - Editor
Robbie Slater, MD - Supervising Editor
Bayar Batmunh, MS - Coordinator

{kind=link}