V6) Chest pain radiating to the back in a patient with uncontrolled hypertension
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a patient with chest pain.
- Review the DDx considerations in a patient with chest pain.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating a patient with chest pain.
History
Physical Exam
Labs
Provisional Diagnosis
Potential Acuity
What is your assessment of the likely acuity for this patient?
First Imaging Study
What is the first imaging study you will order?
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
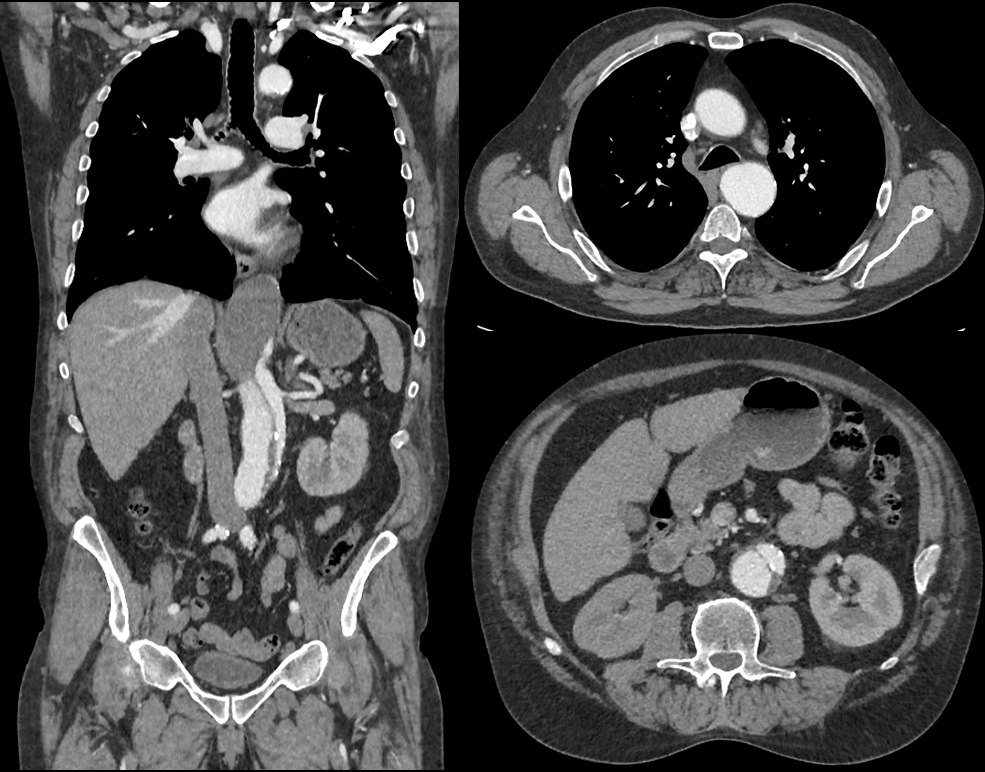
CTA Chest, Abdomen, Pelvis
What best describes the findings on the CT?

Watch our video
Second Imaging Study
What is the next imaging study you will order?
What is your Diagnosis now that you have seen the imaging results?
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
Assessment and Plan
Please provide your assessment and plan for this patient
Lessons Learned:
- Uncontrolled hypertension is a significant risk factor for aortic dissection. Other risk factors include hypertension, atherosclerosis, cardiac or aortic surgical history, aortic aneurysm, connective tissue disorders, and a bicuspid aortic valve.
- Presentation is typically characterized by sudden, severe, tearing chest pain that radiates to the back.
- The first best diagnostic modality is a CTA of the chest, abdomen, and pelvis. Other first tests include transesophageal echocardiography and MRA chest with and without IV contrast.
Socioeconomic Factors: Patients with lower socioeconomic status have been found to have reduced survival following an aortic dissection. Though formal studies do not investigate the matter, it is postulated that patients in lower socioeconomic classes have higher rates of aortic dissection considering the often inadequate blood pressure control in this population.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Contributors:
Jacob Surges, MS3 - Content Contributor
Kevin Pierre, MD - Editor
Robbie Slater, MD - Supervising Editor
Bayar Batmunh - Coordinator

{kind=link}