Retake
N32) Seizures in a hyponatremic patient
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a patient with altered mental status.
- Review the DDx considerations in a patient with altered mental status.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating patients with altered mental status.
History
A 30-year-old male with alcohol use disorder and binge drinking is brought into the ED by a family member due to 2 days of worsening nausea, confusion, vomiting, dizziness, and fatigue. Initial workup revealed a sodium of 114 mEq/L (nl: 135-145mEq/L). He was diagnosed with severe hyponatremia and was started on hypertonic saline at 10mL/hour, which was increased to 55mL/hour the next day. He then developed seizures, altered mental status, dysarthria, and weakness.
Physical Exam
BP: 110/78, HR 86, RR 14 Temp 98 O2 saturation 92%.
Constitutional: Patient appears obtunded.
Neurologic: Hyperreflexia and diminished muscle strength in the bilateral lower extremities.
Labs
Serum sodium: 132 mEq/L (nl: 135-145mEq/L)
Provisional Diagnosis
Select the Dx you believe is most appropriate
Osmotic Demyelination Syndrome is the likely diagnosis given the rapid correction of serum sodium levels following hyponatremia and symptoms of altered mental status and dysarthria. Typically, serum sodium should not be corrected by more than 8-12 mEq/day. Alcohol withdrawal syndrome may present with similar symptoms, but usually develops over the course of several days.
Well done. You were correct
Potential Acuity
What is your assessment of the likely acuity for this patient?
Well done. You were correct
This patient requires urgent workup and management.
First Imaging Study
What is the first imaging study you will order?
Given the high clinical suspicion of osmotic demyelination syndrome, an MRI is an appropriate imaging modality to confirm the diagnosis. MRI can effectively assess for demyelination.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
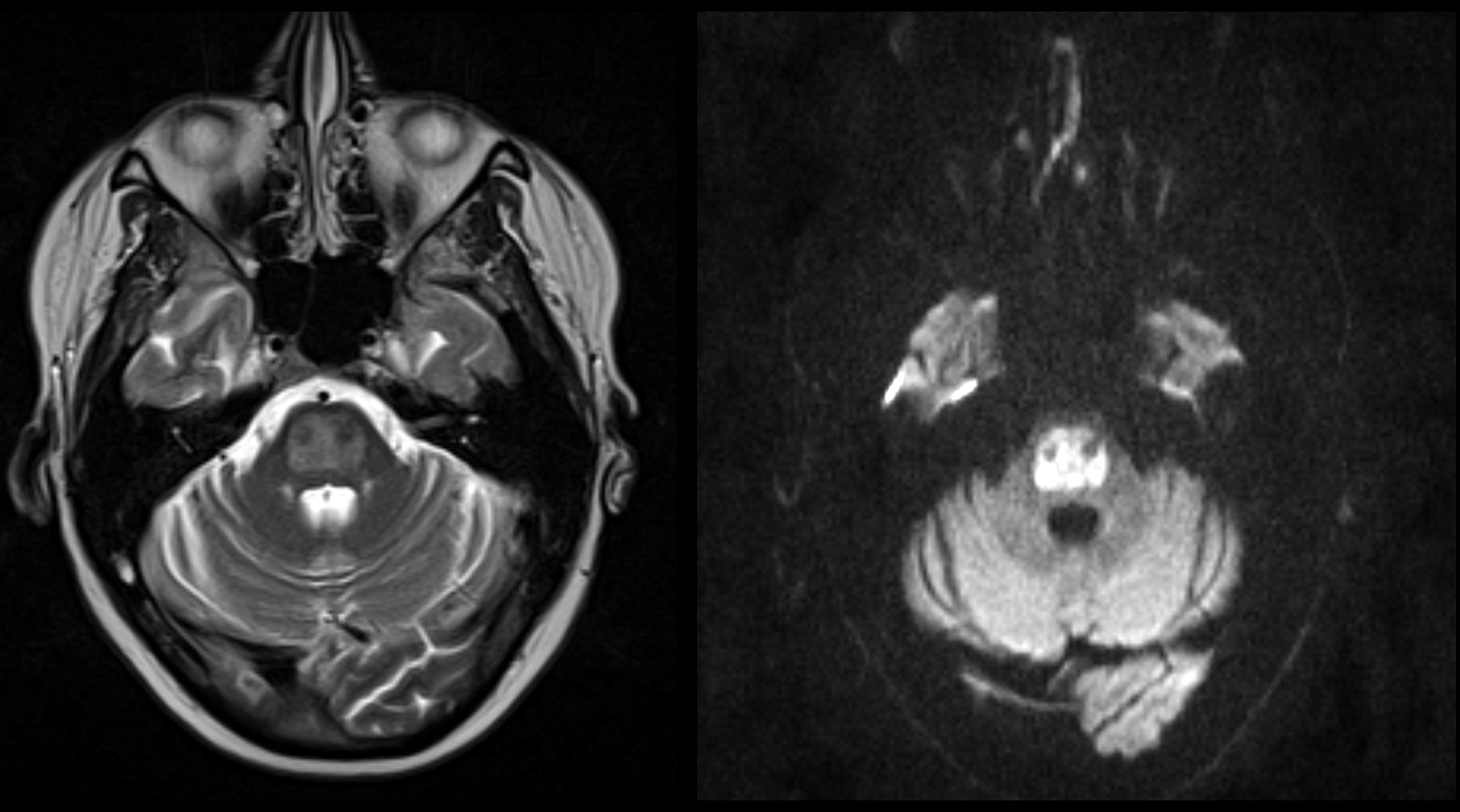
MRI brain
Compared to the rest of the brain parenchyma, most of the pons on the T2 weighted sequence is:
The pons is hyperintense compared to the remainder of the brain parenchyma, suggesting demyelination.
Which structures are largely spared?
The corticospinal tracts are spared, consistent with osmotic demyelination syndrome. This is coined the piglet sign in the superior pons as it resembles the snout of the pig. Inferiorly, it is often coined the trident sign, as it resembles a trident.
View the full study if you'd like to take a look yourself.
What is your Diagnosis now that you have seen the imaging results?
ODS is the correct diagnosis with T2 hyperintensity indicative of bilateral demyelination of the pons. Rapid correction of the patient’s hyponatremia led to the patient presenting with acute signs of encephalopathy and gait abnormalities. Imaging findings typically manifest after the onset of clinical symptoms.
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
The patient requires urgent management.
Assessment and Plan
Please provide your assessment and plan for this patient
The patient is a 30-year-old male with alcohol use disorder who presented with low serum sodium levels, which were corrected too rapidly, resulting in osmotic demyelination syndrome (ODS), confirmed by MRI. The patient should be started on antiepileptics. There is no definitive treatment for ODS besides supportive care. The patient should undergo daily speech and physical therapy and nutrition support. Anti-Parkinsonian drugs may be trialed if he develops secondary parkinsonism. The patient will be closely monitored for any changes in their clinical status and electrolyte levels. The prognosis of ODS is poor, with mortality reported up to 31% in patients. The patient and their family will be counseled on the potential outcomes, and the palliative care physicians should be consulted.
Lessons Learned:
- Osmotic demyelination syndrome (ODS) is a neurological condition that occurs when there is rapid correction of sodium levels at a rate higher than 8-12 mEq/day, leading to demyelination of the pons.
- The increase in serum sodium causes water to be drawn out of neurons, leading to their dehydration and subsequent demyelination.
- It is crucial to correct sodium levels slowly in patients with hyponatremia to prevent the development of ODS, as there is no specific treatment for this condition and it can be fatal.
- MRI is the imaging modality of choice for diagnosing ODS, and it often reveals positive findings after the onset of clinical symptoms, which may take up to 2 weeks.
- Classic MRI findings of ODS include hyperintensity in the pons on T2/FLAIR and DWI, hypo-intensity of the pons on T1, and the piglet and trident signs, reflecting sparing of the peripheral pons and corticospinal tract.
- In ODS, the peripheral pons, corticospinal tract, and periventricular regions, are typically spared from demyelination.
Socioeconomic Factors: Patients with ODS often present with mild neurological symptoms. In regions where healthcare access is limited, this can result in misdiagnosis or inadequate treatment.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Next


{kind=link}