Retake
N27) Headache and altered mental status in an immunocompromised patient
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a patient with confusion.
- Review the DDx considerations in a patient with confusion.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating patients with confusion.
History
A 33-year-old woman with untreated HIV presents with a 3-day history of progressive headache, fever, and altered mental status culminating in a witnessed seizure. The headache is described as worsening, associated with nausea, and her partner reports episodes of confusion and disorientation. Past medical history is significant for IV drug use. Her HIV diagnosis was made a year ago, but she opted for homeopathic remedies rather than antiretroviral therapy.
Physical Exam
Vitals: BP 125/83, HR 105, RR 14, Temp 101F, SpO2 98% on room air. BGL: 78mg/dL.
Neurological exam: she is oriented to person but not place or time. Left upper and lower extremity strength at 4+/5, with diminished sensation.
Labs
CD4 count = 64 cells/uL (Reference range: 500-1500 cells/uL)
Provisional Diagnosis
Select the Dx you believe is most appropriate
The patient's history of untreated HIV with a CD4 count of 64 cells/uL, and clinical features including a fever, seizure, with focal neurologic deficits suggest a CNS infection such as toxoplasmosis, which can occur in severely immunocompromised HIV patients. However, CNS lymphoma, a type of malignancy associated with HIV, cannot be excluded at this stage.
Well done. You were correct
Potential Acuity
What is your assessment of the likely acuity for this patient?
Well done. You were correct
The patient requires urgent workup and management considering their new onset seizures and with concern for an intracranial infection in the setting of severe immunocompromise.
First Imaging Study
What is the first imaging study you will order?
A CT head with and without contrast is an appropriate initial imaging modality in a patient presenting with acute onset seizures with concern of an intracranial mass. It is quickly obtainable and can rule out immediately life-threatening conditions.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
CT head
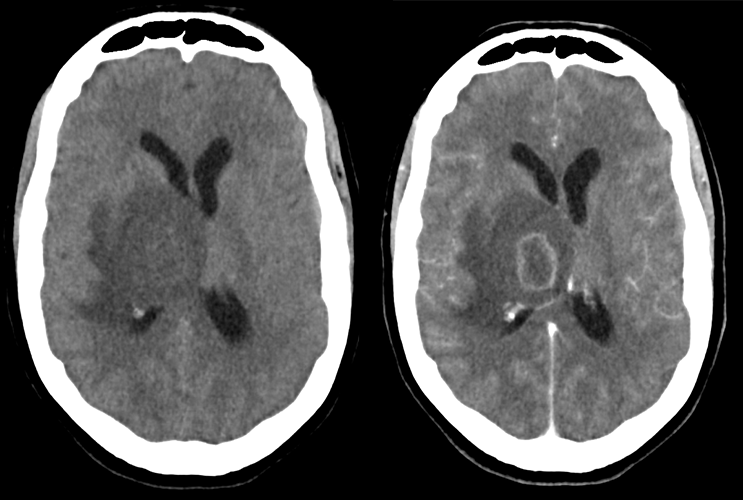
The lesion demonstrates:
The non-contrast CT (Image 2) reveals a large intraparenchymal lesion. It is surrounded by vasogenic edema causing midline shift. The contrast-enhanced CT (Image 1) clearly differentiates the lesion from normal brain tissue and shows its ring-enhancement.
The lesion is primarily centered over the:
The lesion is primarily centered over the right thalamus.
View the full study if you'd like to take a look yourself.
Second Imaging Study
What is the next imaging study you will order?
An MRI with and without contrast is an appropriate additional imaging modality as it can detect additional lesions not apparent on the CT and offer distinguishing characteristics between CNS lymphoma and toxoplasmosis.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
MRI brain
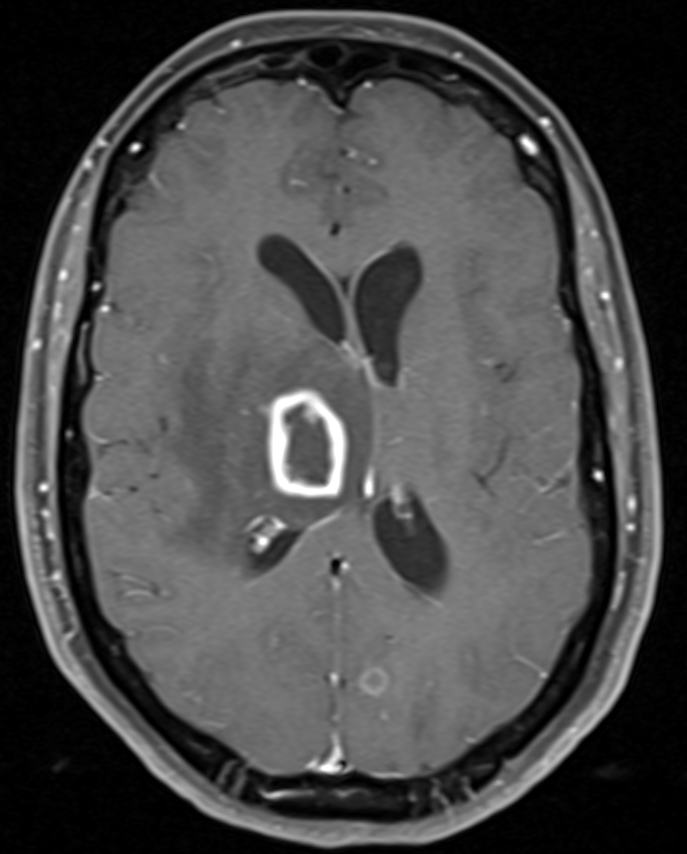
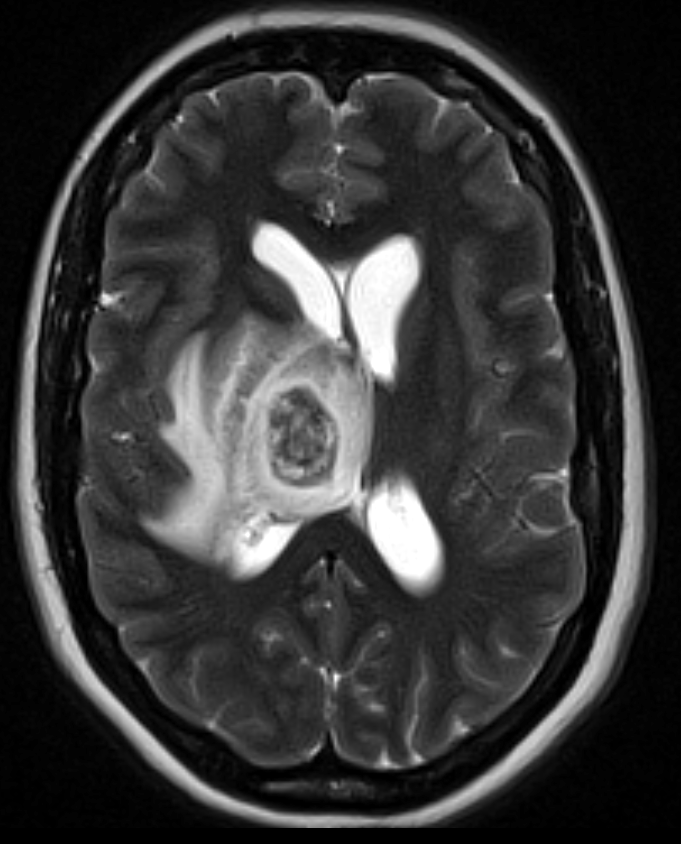
How many lesions are there?
There are multiple lesions. There is a large lesion in the right thalamus. The contrasted images also show a lesion in the left parieto-occipital region.
The ring-enhancing lesion results in:
There is vasogenic edema surrounding the lesion. Vasogenic edema typically presents in a more localized, perilesional pattern, and tends to respect the gray-white matter junction, outlining the cortex due to its predominance in the white matter. Cytotoxic edema, on the other hand, is more uniform and diffuse, and does not spare the gray matter, leading to a loss of differentiation between gray and white matter on imaging.
View the full study if you'd like to like a look yourself
Third Imaging Study
What is the next imaging study you will order?
No further imaging is needed. The lesion has been well-characterized with imaging. Further imaging would not change management.
What is your Diagnosis now that you have seen the imaging results?
This patient with advanced HIV, neurological symptoms, fever, and multiple ring-enhancing brain lesions likely has cerebral toxoplasmosis, a common AIDS-defining neurological disorder. The MRI reveals multiple peripherally enhancing lesions without definitive diffusion restriction, a pattern more consistent with toxoplasmosis. In contrast, CNS lymphoma usually presents as a singular lesion and tends to show diffusion restriction.
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
This severely immunocompromised patient has multiple intracranial lesions with concern for progressive disease. They therefore require prompt treatment.
Assessment and Plan
Please provide your assessment and plan for this patient
This is a 33-year-old female patient with uncontrolled HIV presenting with focal neurologic deficits, seizures, altered mental status, and fever. The MRI findings show multiple peripherally enhancing lesions without definitive diffusion restriction, which suggests a diagnosis of cerebral toxoplasmosis.
The patient should be started empirically on toxoplasmosis treatment, which usually involves a combination of pyrimethamine, sulfadiazine, and leucovorin. We will also counsel her on the importance of antiretroviral therapy and initiate antiseizure prophylaxis. We should consult Infectious Diseases and Neurology for continued management. She should be on continued on prophylaxis against toxoplasmosis with TMP-SMX as her CD4 count < 100.
Lessons Learned:
- Cerebral toxoplasmosis primarily affects severely immunocompromised individuals. It a common neurological disorder associated with AIDS and affects those with a CD4 count < 100.
- It is caused by Toxoplasma gondii, an intracellular protozoan. Infection is prevalent worldwide, but it is typically asymptomatic.
- In adults, it is commonly transmitted via oral ingestion of oocysts from cat feces or raw meat.
- Clinical features include fever, headache, focal neurologic deficits, seizures, and altered mental status.
- Initial imaging usually involves a CT scan, which typically reveals hypodense, ring-enhancing lesions with vasogenic edema, mostly in the basal ganglia and corticomedullary junction.
- MRI, while variable in intensity, helps in better characterization of lesions and typically exhibits ring-enhancement with contrast and no diffusion restriction.
- CNS lymphoma presents in the same population but tends to have a single or few lesions with homogenous enhancement.
- Management involves antitoxoplasmic therapy (pyrimethamine, sulfadiazine, and leucovorin) alongside appropriate antiretroviral treatment. Prophylaxis with TMP-SMX is recommended for patients with a CD4 count below 100.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Next


{kind=link}
{kind=link}
{kind=link}