Retake
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a patient with left lower abdominal pain.
- Review the DDx considerations in abdominal pain scenarios.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating patients with lower abdominal pain.
History
A 66 year old male has a history of abrupt onset of acute lower abdominal pain. He denies nausea and vomiting but is anorexic and only tolerating liquids. He has had no BM since the onset of symptoms. He is currently on chemotherapy for follicular non-Hodgkin's lymphoma. He is also a diabetic. Previous lumbar laminectomy.
Physical Exam
BP 128/76, HR 96, RR 22, temp 37.4. Heart RRR, lungs are clear. The abdomen is tender to palpation in the left lower quadrant, no rebound. Abdomen is not distended. Bowel sounds are normal.
Labs
CBC: white count 9.2, Hb 15.9, Hct 46. Normal platelets and INR. Oxygen sat 97% on room air. BMP normal. LFTs and lipase are normal. Glucose 150. UA negative.
Provisional Diagnosis
Select the Dx you believe is most appropriate
Acute cholecystitis would likely cause RUQ pain. A perforated ulcer would likely cause peritoneal signs such as rebound, abdominal rigidity, pain with movement. Appendicitis and diverticulitis are possible for lower abdominal pain, even if not localized to the RLQ or LLQ, respectively.
Well done. You were correct
Potential Acuity
What is your assessment of the likely acuity for this patient?
Well done. You were correct
Given the patient's age and history, the etiology of his abdominal pain needs to be further evaluated.
First Imaging Study
What is the first imaging study you will order?
The patient likely does not have cholecystitis. An acute abdominal series may reveal free air in the abdomen, dilated bowel, pneumatosis, portal venous gas, or be normal. A CT scan is a reasonable first step if clinical suspicion of pathology is high. For this patient, the abdominal series was initially obtained in the ED.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
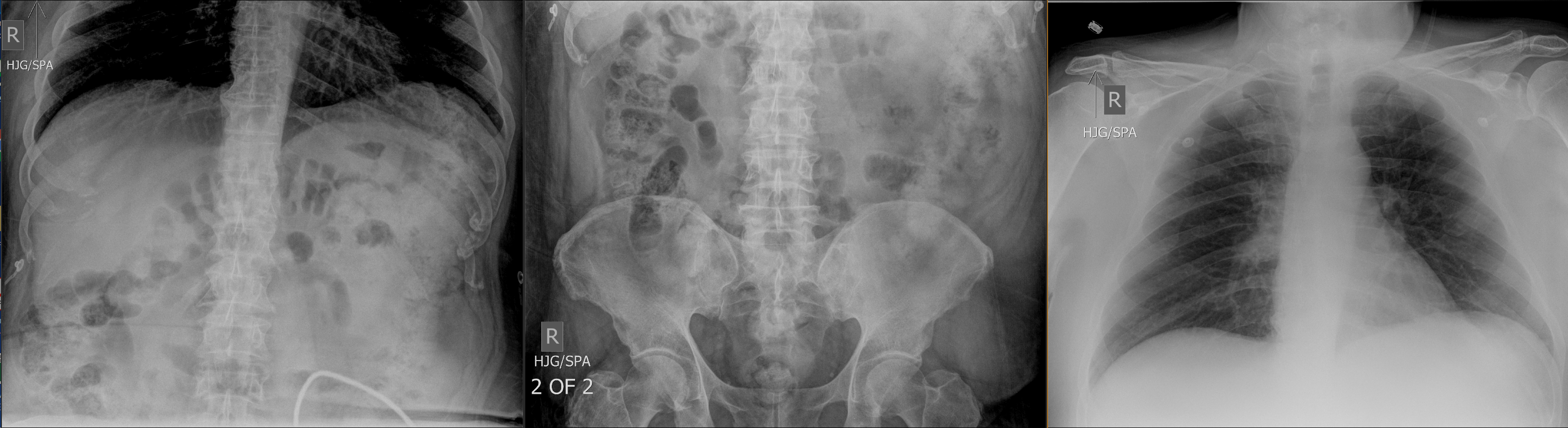
Acute abdominal series
Look at the patient's acute abdominal series. There is evidence of free air from hollow viscus perforation.
No, this patient does not have pneumoperitoneum.
View the full study if you'd like to take a look yourself.
Second Imaging Study
What is the next imaging study you will order?
The CT scan would be the next appropriate imaging study.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
Abdomen/pelvis CT
Selected CT images show inflammation in the RLQ likely from appendicitis.
No, there is inflammation in the left lower quadrant.
View the full study if you'd like to like a look yourself
What is your Diagnosis now that you have seen the imaging results?
There is diverticulosis of the sigmoid colon. The thickening with fat stranding around the sigmoid are indicative of inflammation from diverticulitis. There is no fluid collection to suggest abscess.
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
The patient will need IV antibiotic treatment and surgical consult.
Assessment and Plan
Please provide your assessment and plan for this patient
Diverticulitis without abscess or free air. The patient will be kept NPO initially and treated conservatively with IVFs and antibiotics. Serial abdominal exams. Surgery will be consulted.
CT abdomen/pelvis review
Lessons Learned: Uncomplicated diverticulitis can be treated conservatively with antibiotics. A small, contained abscess or microperforation can likely be managed conservatively. An abscess may be amenable to drainage by Interventional Radiology. A perforation with generalized pneumoperitoneum or extensive abscess formation would likely require surgical intervention.
Socioeconomic Factors: This patient was able to be treated conservatively and did not require home health services. He continued to be followed by the Oncology service for his NHL treatment.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Next


{kind=link}
{kind=link}