A23) Blunt trauma
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a patient presenting after trauma.
- Review the DDx considerations in a patient presenting after trauma.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating a patient presenting after trauma.
History
Physical Exam
Labs
Provisional Diagnosis
Potential Acuity
What is your assessment of the likely acuity for this patient?
First Imaging Study
What is the first imaging study you will order?
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
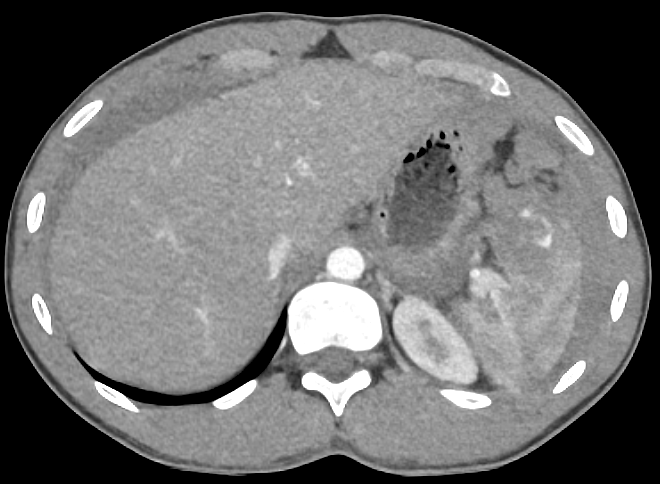
CT trauma series
There is free intraperitoneal air
There is evidence of splenic injury on the venous phase CT
There is active extravasation of blood on the arterial phase CT
There is hemoperitoneum on the arterial phase CT

Watch our video
Second Imaging Study
What is the next imaging study you will order?
What is your Diagnosis now that you have seen the imaging results?
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
Assessment and Plan
Please provide your assessment and plan for this patient
Lessons Learned:
- A splenic injury is likely to occur following blunt trauma to the abdomen such as motor vehicle accidents, sport injuries, or other violent causes such as fist blows or stabbings. Patients with recent history of EBV are at increased risk for spontaneous atraumatic rupture.
- The diagnosis should be suspected in someone who experienced blunt abdominal trauma, with either diffuse tenderness or tenderness in the LUQ, Kher’s sign (pain in left shoulder and neck worse with inspiration), and a seatbelt sign (abdominal wall ecchymosis).
- The first best diagnostic modality is a body trauma CT with IV contrast. It evaluates for active bleeding and presence of hemoperitoneum. Additionally, it can be used to determine the grading of the laceration, which can guide the treatment plan.
- High grade splenic lacerations (grades 4 and 5) in hemodynamically unstable patients likely require surgical intervention.
- This case emphasizes the importance of the ATLS protocol. Had this hemodynamically unstable patient undergone management per this protocol, they would have likely gone to surgery prior to CT scanning had the FAST exam shown free intraperitoneal fluid.
Socioeconomic Factors: Racial, ethnic, and socioeconomic disparities exist in trauma patients. For example, uninsured patients undergo less angioembolizations and are less likely to undergo nonoperative treatment. These patients also have higher mortality.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Contributors:
Seyedeh Mehrsa Sadat Razavi, MS2 - Content Contributor
Kevin Pierre, MD - Editor
Robbie Slater, MD - Supervising Editor
Bayar Batmunh, MS - Coordinator

{kind=link}
{kind=link}
{kind=link}
{kind=link}